Thyroid eye disease (TED), also known as Graves’ orbitopathy or thyroid-associated ophthalmopathy, is an autoimmune inflammatory disorder affecting the tissues surrounding the eyes, including the extraocular muscles, orbital fat, connective tissue, and eyelids. It occurs most commonly in people with Graves’ disease, although it can also develop in individuals with normal or underactive thyroid function. TED is a rare, debilitating disease that can cause eye dryness and redness, eyelid swelling or retraction, bulging eyes (proptosis), double vision, and, in severe cases, vision impairment.
While TED is common among individuals with GD, with an estimated global prevalence of 40%, there are a limited number of studies comparing the incidence or prevalence of TED among different ethnic groups.
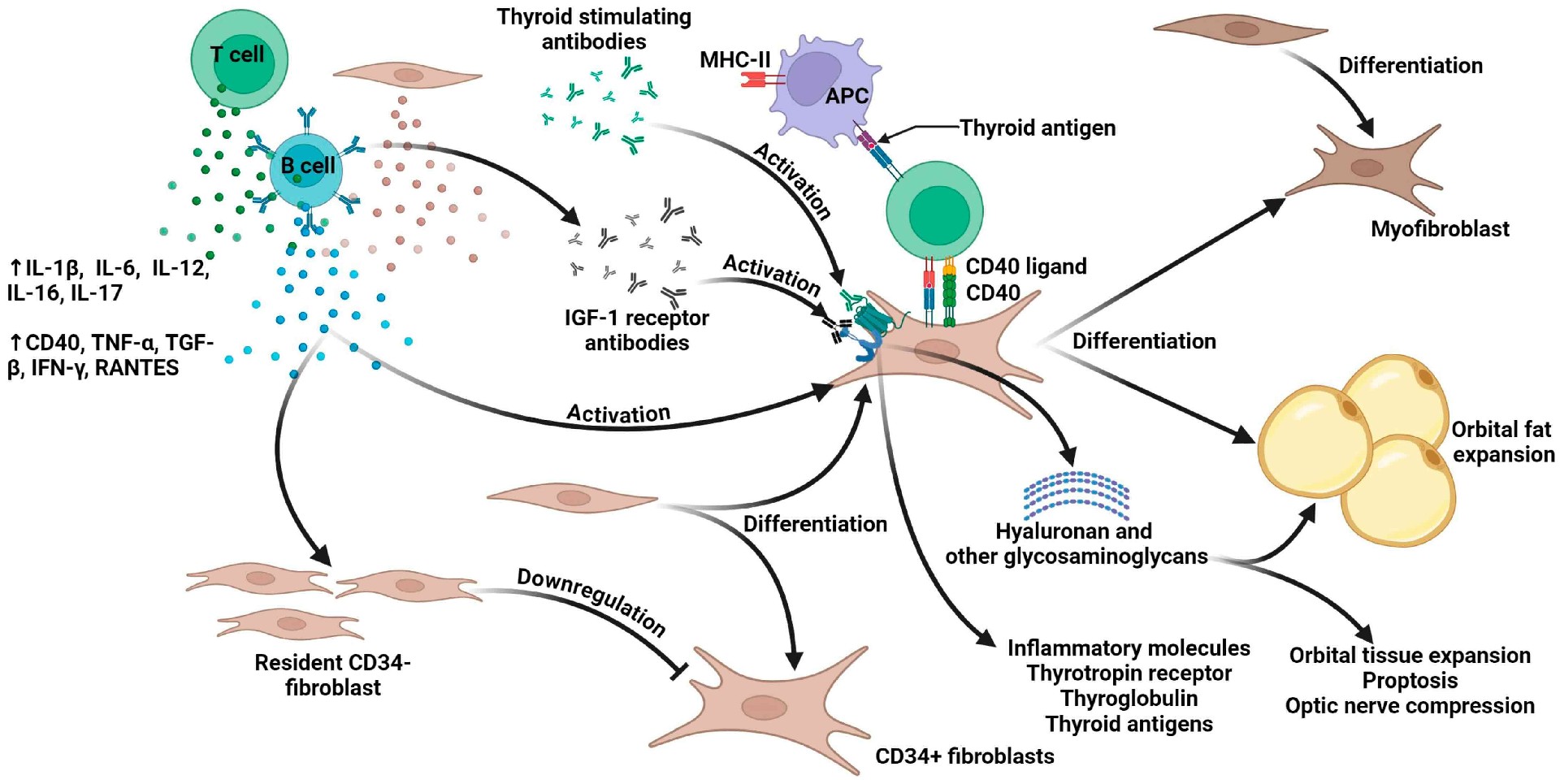
Treatment for thyroid eye disease is selected according to disease activity, severity, predominant clinical features, patient comorbidities, and treatment availability. Teprotumumab (Tepezza), approved in 2020 as the first FDA-approved therapy specifically for TED, is a fully humanized monoclonal antibody that inhibits insulin-like growth factor-1 receptor signaling. IGF-1R is a widely expressed transmembrane receptor that regulates growth, cell survival, differentiation, and tissue homeostasis through pathways including PI3K-AKT and Ras-MAPK, raising the possibility of systemic adverse effects when it is therapeutically inhibited. In TED, crosstalk between IGF-1R and TSHR activates orbital fibroblasts, promoting cytokine and glycosaminoglycan production, immune-cell infiltration, adipogenesis, muscle enlargement, edema, and fibrosis, making this signaling network an important therapeutic target.

Teprotumumab N01, was also approved as Sycume in China for TED as the nation’s first and the world’s second approved IGF-1R antibody drug in March 2025.
Most recently, in June 2026, the FDA approved Lumvoa (veligrotug-vvze), formerly VRDN-001, providing a second IGF-1R-targeting mAb for both active and chronic TED. Veligrotug also binds to membrane-bound IGF-1R and inhibits its activity, thereby preventing the interaction with its natural ligand IGF-1 and the subsequent activation of PI3K/AKT signal transduction. Approval was supported by the Phase 3 THRIVE and THRIVE-2 trials, in which Lumvoa produced rapid and durable improvements in proptosis, diplopia, inflammation, and other key symptoms across both active and chronic TED.

Tocilizumab, a humanized IL-6 receptor mAb approved for several inflammatory diseases, is also a potential off-label in selected patients with active, moderate-to-severe TED, particularly after an inadequate response to glucocorticoids. By inhibiting IL-6 signaling, tocilizumab may reduce orbital fibroblast activation, inflammation, glycosaminoglycan production, tissue swelling, proptosis, and impaired eye movement. A meta-analysis of seven studies involving 161 patients found significant improvements in clinical activity score, proptosis, and diplopia among patients with steroid-resistant active disease. However, the evidence was based largely on small cohort studies and only one randomized controlled trial, while serious adverse-event rates varied, indicating that larger controlled studies are still needed.
Following the clinical validation of IGF-1R inhibition by teprotumumab, researchers are looking at subcutaneous IGF-1R inhibition, which could reduce infusion-center dependence and potentially support administration at home.
Elegrobart is a half-life-extended anti-IGF-1R mAb being developed for infrequent subcutaneous administration through an autoinjector with plans to seek FDA approval in 2027.
Teprotumumab itself may also soon be administered subcutaneously instead of intravenously, with positive Phase 3 results for a subcutaneous formulation delivered through an on-body injector.
Meanwhile, lonigutamab represents another subcutaneous anti-IGF-1R approach. Unlike other anti-IGF-1R treatments, lonigutamab binds to a distinct epitope, triggering rapid receptor internalization and degradation of the receptor complex.
Several programs are targeting other components of TED pathogenesis. The most advanced is satralizumab, a recombinant IL-6 receptor monoclonal antibody already marketed as Enspryng for neuromyelitis optica spectrum disorder. By preventing IL-6 from binding to its receptor, it reduces proinflammatory and profibrotic signaling. Roche reported improvements across proptosis, diplopia and inflammatory outcomes in the Phase 3 SatraGO program, and the FDA granted the TED application Priority Review in June 2026, with a decision expected by October 15, 2026.
Other than that, LASN01, a fully human anti-IL-11 receptor mAb, is being evaluated in Phase 2 as an approach to reducing fibro-inflammatory signaling, orbital fibroblast proliferation, hyaluronan production and fibrosis. Pacibekitug, a long-acting anti-IL-6, fully human IgG2 mAb, is being studied in a Phase 2b trial using three subcutaneous injections given eight weeks apart.
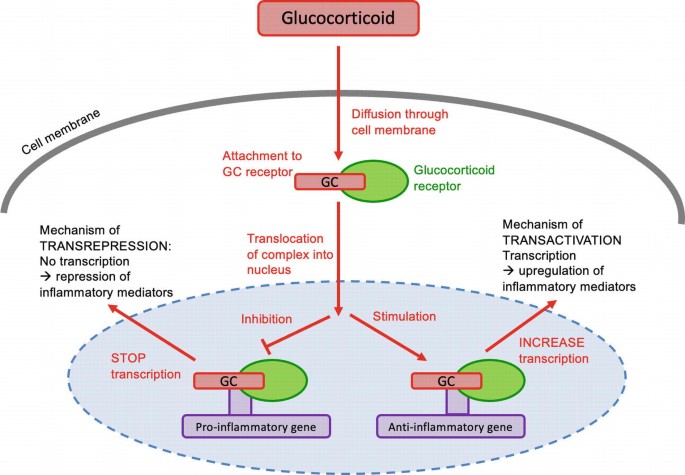
Despite this expanding pipeline, targeted therapies have not replaced glucocorticoids or surgery. Intravenous glucocorticoids remain an established treatment for active, moderate-to-severe inflammatory TED, particularly when inflammation and soft-tissue involvement are the dominant features. Urgent glucocorticoid treatment or orbital decompression may be required for sight-threatening disease, while decompression, strabismus and eyelid surgery remain important for persistent structural abnormalities after the disease becomes inactive. Treatment is thus becoming more individualized.
Biointron’s Q2 2026 Antibody Industry Trends report aims to explore the events a……
Artificial intelligence is changing how researchers think about antibody discove……
Seasonal influenza causes an estimated one billion infections, 3-5 million sever……