Neurodegenerative diseases such as Alzheimer’s disease (AD), Parkinson’s disease, amyotrophic lateral sclerosis (ALS), and Huntington’s disease represent an escalating global health challenge, driven by an aging population and the lack of effective disease-modifying therapies. Despite extensive research, most therapeutic candidates fail to achieve sufficient CNS exposure due to the restrictive blood–brain barrier (BBB), which blocks over 98% of small molecules and nearly all biologics from entering the brain parenchyma. This barrier, formed by endothelial cells, pericytes, and astrocytic end-feet, maintains neural homeostasis but limits drug delivery to the CNS.
The BBB was once viewed as impenetrable but is now recognized as a dynamic interface that can be selectively and safely engaged for therapeutic delivery. This shift has driven strategies to overcome the barrier via physical modulation, biochemical transport, or alternative administration routes. Among these, receptor-mediated transcytosis (RMT) has gained prominence for harnessing endogenous transport systems such as transferrin or insulin receptor pathways to shuttle macromolecules across the BBB. Other methods are being researched, such as focused ultrasound (FUS), ligand-decorated nanoparticles, exosomes, and lipid-based carriers. Once considered speculative, these approaches have entered preclinical and early clinical testing, supported by advances in quantitative imaging.

The blood-brain barrier (BBB) is a specialized vascular interface that tightly regulates molecular exchange between the bloodstream and the central nervous system (CNS). It is formed by endothelial cells connected through tight and adherens junctions, supported by pericytes and astrocytic end-feet comprising the neurovascular unit. This architecture maintains CNS homeostasis by allowing controlled passage of nutrients, hormones, and metabolites while excluding most xenobiotics and macromolecules. However, these same protective mechanisms create a major pharmacological bottleneck, particularly for biologics such as antibodies, enzymes, and nucleic acid-based therapeutics exceeding 400-500 Da.
Barrier selectivity arises from both physical and biochemical features. Tight junctions restrict paracellular diffusion, while transport proteins and efflux pumps such as ATP-binding cassette (ABC) transporters actively remove compounds entering endothelial cells. The low rate of transcytosis across brain capillaries further limits macromolecule passage. As a result, only about 0.1% of a systemically administered monoclonal antibody reaches the brain parenchyma, explaining the high doses and dose-dependent side effects of antibody-based Alzheimer’s disease (AD) therapies.
BBB dysfunction varies across disease states. In neurodegenerative diseases such as AD, vascular pathology, amyloid accumulation, and neuroinflammation can alter endothelial integrity and transport behavior, often increasing permeability in heterogeneous and spatially restricted ways. This variability complicates generalized delivery strategies and underscores the need for patient-specific approaches in CNS pharmacotherapy.

Receptor-mediated transcytosis (RMT) is a strategy for transporting large biologics across the blood-brain barrier (BBB). It leverages endogenous pathways that deliver essential macromolecules such as transferrin and insulin into the brain. By engineering antibodies or biologics to engage these receptors, researchers have increased brain uptake while maintaining BBB integrity and minimizing off-target effects.
RMT involves internalization of receptor-ligand complexes at the luminal surface of endothelial cells, vesicular trafficking, and release at the abluminal side. The transferrin receptor (TfR1), insulin receptor (InsR), and neonatal Fc receptor (FcRn) are the most studied systems.
TfR1 is the main target for BBB transport platforms. High-affinity or multivalent binding can cause receptor clustering and degradation, whereas moderate-affinity, monovalent binding promotes recycling and productive transport. InsR systems offer broader access but risk affecting glucose metabolism, while FcRn enables bidirectional antibody movement across the BBB.
Optimizing these interactions requires balancing affinity, valency, and trafficking kinetics. pH-sensitive antibodies that dissociate under acidic conditions enhance recycling and avoid degradation.
TfR1-targeted bispecific antibodies have advanced rapidly toward clinical use. By fusing an anti-TfR1 domain to a therapeutic antibody, these constructs achieve higher and more uniform brain distribution. In Alzheimer’s disease (AD) models, TfR1-bispecific antibodies clear plaques at lower doses, improving pharmacodynamic efficiency.
Clinical candidates such as Roche’s Trontinemab (a TfR1-bispecific derivative of Gantenerumab) show rapid amyloid clearance and reduced amyloid-related imaging abnormalities (ARIA), reflecting improved distribution. Related transport vehicle (ATV) systems, such as ATVcisLALA:Aβ, apply Fc-engineering to retain microglial activation while limiting systemic side effects.
Imaging and single-cell RNA sequencing reveal that TfR1-targeted ATVs localize mainly to neurons and astrocytes, while CD98hc-targeted constructs show broader astrocyte and microglia uptake. Findings in non-human primates confirm strong translational potential.

RMT design now extends to enzymes, antisense oligonucleotides (ASOs), and viral vectors through incorporation of TfR1- or CD98hc-binding modules. Cross-species single-domain antibodies (VHHs) recognizing conserved TfR1 epitopes serve as efficient shuttles that do not disrupt endogenous transferrin binding. Data-driven screening platforms evaluate thousands of constructs in vivo. Coupled with machine learning, these datasets identify features that enhance BBB penetration and brain distribution.

Crossing the BBB is only the first step. Once in the CNS, distribution and retention shape pharmacological activity. TfR1-targeted antibodies enter rapidly but degrade faster, whereas CD98hc-targeted molecules traffic slowly yet persist longer.
Current strategies aim to balance entry and stability using dual-target designs, anchoring domains, and pH-dependent receptor interactions to promote recycling. Integrating BBB transport, parenchymal diffusion, and systemic pharmacokinetics into unified models will enable more accurate prediction of exposure and dosing. Collectively, these advances shift the focus from BBB penetration alone to a holistic framework linking transport, distribution, pharmacodynamics, and safety.

While receptor-mediated transcytosis (RMT) is the leading approach for transporting biologics into the brain, several complementary strategies aim to bypass or transiently modulate the blood-brain barrier (BBB). These include physical disruption, nanocarrier systems, and direct nose-to-brain delivery, with each expanding therapeutic access to the central nervous system (CNS) while maintaining safety and translational feasibility.
Focused Ultrasound (FUS) with Microbubbles: Focused ultrasound (FUS), paired with microbubbles, transiently opens BBB tight junctions to allow antibody entry. In Alzheimer’s models, FUS alone reduces amyloid plaques, while co-delivery with antibodies enhances clearance. Human trials show MRI-guided FUS can safely and reversibly open targeted regions. Challenges include potential inflammation and uncertainty around optimal dosing, but continued refinements make FUS a promising adjunct for localized biologic delivery.
Nanoparticle and Exosome-Based Carrier: Nanoparticles and engineered exosomes can encapsulate therapeutics and be functionalized with BBB-targeting ligands (e.g., transferrin or LRP1). They show preclinical success in improving CNS drug accumulation and stability. However, issues with reproducibility, scalability, and immunogenicity limit clinical progress. The actual proportion crossing the BBB remains low, underscoring the need for quantitative imaging tools to validate delivery. Still, their modularity allows for future integration with other delivery methods.
Intranasal and Localized Delivery: Localized routes such as the Minimally Invasive Nasal Depot (MIND) can bypass the BBB by delivering antibodies directly to the olfactory region for sustained brain release. In preclinical models, MIND reduced neuroinflammation without systemic side effects and was well tolerated. Though penetration depth is limited, intranasal approaches offer practical, noninvasive options for chronic or cortical CNS diseases.

Advances in blood-brain barrier (BBB) therapeutics increasingly rely on tools that quantify and predict molecular transport across the neurovascular unit. Modern imaging, in vitro models, and computational design frameworks now offer precise, real-time insight into BBB permeability and drug behavior.
Positron emission tomography (PET), particularly ^89Zr-immunoPET, enables noninvasive tracking of antibody biodistribution and receptor engagement in living subjects. Studies show that higher transferrin receptor affinity enhances BBB transcytosis at tracer doses, refining our understanding of dose-dependent transport. ImmunoPET bridges molecular design and pharmacokinetics, providing essential validation of BBB delivery in vivo
Three-dimensional (3D) and microfluidic BBB models replicate realistic cell interactions and flow conditions, outperforming traditional monolayers. For example, organ-on-a-chip and brain organoids enable studies of permeability, receptor transport, and disease-related dysfunctions like inflammation or amyloid buildup. Despite challenges in reproducibility, standardization efforts and hybrid models combining chips with neural organoids are enhancing translational predictability.
High-throughput and machine learning-based systems are reshaping BBB drug discovery. Platforms like Manifold’s mCode™ screen thousands of antibody variants in vivo, generating biodistribution and brain-uptake data that feed into predictive algorithms. This accelerates identification of structural motifs and receptor targets that drive efficient BBB penetration.

The convergence of antibody engineering, molecular modeling, and receptor biology is reshaping the future of brain-targeted therapeutics. Advances in receptor-mediated transcytosis, bispecific antibody design, and AI-enabled discovery are transforming the blood–brain barrier from a delivery obstacle into an integrated part of therapeutic strategy. As these technologies move from concept to clinic, the ability to produce customized antibodies optimized for affinity, valency, and modular fusion with transport vehicles, will be essential for success.
Biointron’s antibody discovery and developability platforms are uniquely positioned to support this next generation of CNS therapeutics. With rapid antibody generation, bispecific engineering, and manufacturability assessment capabilities, Biointron enables researchers to efficiently translate molecular concepts into clinically viable brain-penetrant antibodies. By bridging innovation in design with practical development expertise, Biointron helps accelerate the path toward safe and effective biologics that can reach targets once considered inaccessible within the brain.
Biointron’s Q2 2026 Antibody Industry Trends report aims to explore the events a……
Seasonal influenza causes an estimated one billion infections, 3-5 million sever……
Artificial intelligence can now help researchers analyze antibody sequences, pre……
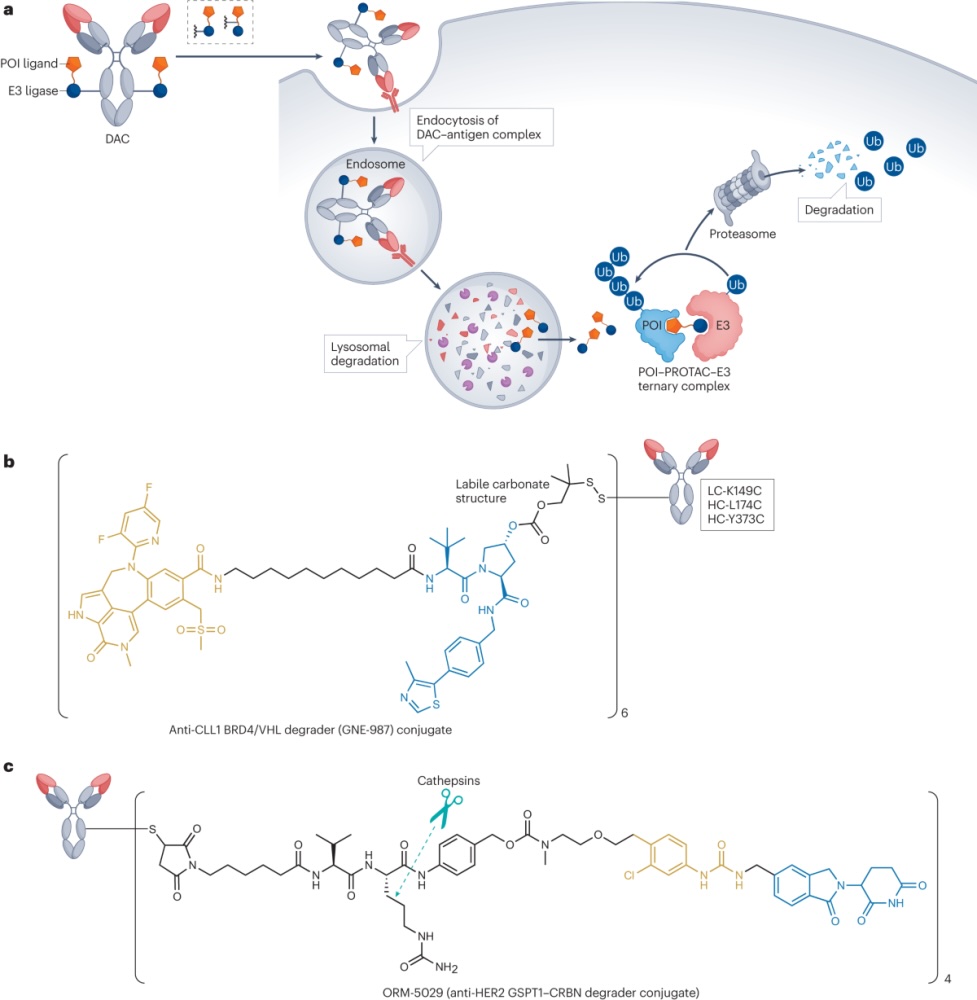
Degrader-antibody conjugates, or DACs, combine the targeting ability of antibodi……