Multiple myeloma (MM) is a hematologic malignancy characterized by the clonal proliferation of malignant plasma cells within the bone marrow, often resulting in anemia, bone lesions, hypercalcemia, and renal dysfunction. Despite recent therapeutic advances, MM remains incurable, and most patients ultimately experience relapsed or refractory disease (R/R MM). A prominent therapeutic target in MM is B-cell maturation antigen (BCMA), a cell-surface receptor expressed almost exclusively on plasma cells and malignant myeloma cells, making it a highly specific and clinically actionable target for immunotherapies. Recent developments in BCMA-directed antibody therapies underscore a shift in the treatment paradigm for R/R MM.
On April 28, 2025, the European Commission approved linvoseltamab (Lynozyfic) for adults with R/R MM who have undergone at least three prior therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody. Linvoseltamab is a bispecific antibody targeting BCMA and CD3, facilitating T-cell mediated cytotoxicity against MM cells. In the pivotal LINKER-MM1 trial (n=117), linvoseltamab achieved a 71% overall response rate (ORR), with 50% of patients reaching complete response (CR) or better. Importantly, the minimal residual disease (MRD) negativity rate among these responders was 41%, with a median duration of response (DOR) of 29 months. The response-adapted dosing regimen allowing for every-four-week administration post-VGPR offers a significant advancement in convenience and treatment sustainability.

Belantamab mafodotin (Blenrep), a BCMA-directed antibody-drug conjugate (ADC), has received UK MHRA approval for use in combination regimens. These include Blenrep with bortezomib and dexamethasone (BVd) or with pomalidomide and dexamethasone (BPd), following at least one prior line of therapy. The DREAMM-7 and DREAMM-8 trials demonstrated superior efficacy over standard-of-care comparators, with the BVd regimen achieving a median PFS of 36.6 months (vs. 13.4 months; HR=0.41) and significantly improved OS. These findings establish Blenrep’s efficacy in combination therapy despite its earlier withdrawal as a monotherapy in the U.S. due to the DREAMM-3 outcome. Ocular toxicity, a class-related effect, was effectively managed via dosing adjustments.

ISB 2001, a trispecific antibody engaging BCMA, CD38, and CD3, has been granted Fast Track Designation by the FDA for patients with R/R MM who have received at least three prior lines of therapy. Engineered for enhanced tumor targeting and reduced off-tumor toxicity, ISB 2001 demonstrated an 83% ORR in dose levels 3-7 during a phase 1 trial, with a CR rate of 22% and VGPR of 50%. Responses were observed even in patients previously treated with CAR T-cells or bispecific antibodies, indicating potential utility in heavily pretreated and refractory populations. No dose-limiting toxicities were observed, and all cytokine release syndrome (CRS) events were grade 1 or 2.

Meanwhile, a multi-institutional retrospective study assessed IVIG prophylaxis in 225 patients treated with BCMA-directed bispecific antibodies, including teclistamab. Those who received IVIG prior to their first infection had significantly longer infection-free survival (7.7 vs. 3 months for all-grade; 14 vs. 7.5 months for ≥grade 3 infections) and improved progression-free and overall survival. IVIG prophylaxis was independently associated with a 63% reduction in mortality risk (HR=0.37, p=0.021). Given the humoral immunodeficiency induced by BCMA-targeted BsAbs, especially teclistamab, these findings advocate for preemptive IVIG administration as a strategy to sustain treatment continuity and enhance outcomes.

These collective findings reinforce BCMA as a central target in R/R MM and demonstrate the growing sophistication of immunotherapeutic approaches. Approvals of new bispecific and ADC combinations, the clinical advancement of trispecific formats, and the incorporation of adjunctive therapies like IVIG prophylaxis reflect an expanding and increasingly personalized therapeutic armamentarium aimed at prolonging remission and improving survival outcomes in this challenging disease.
Biointron’s Q2 2026 Antibody Industry Trends report aims to explore the events a……
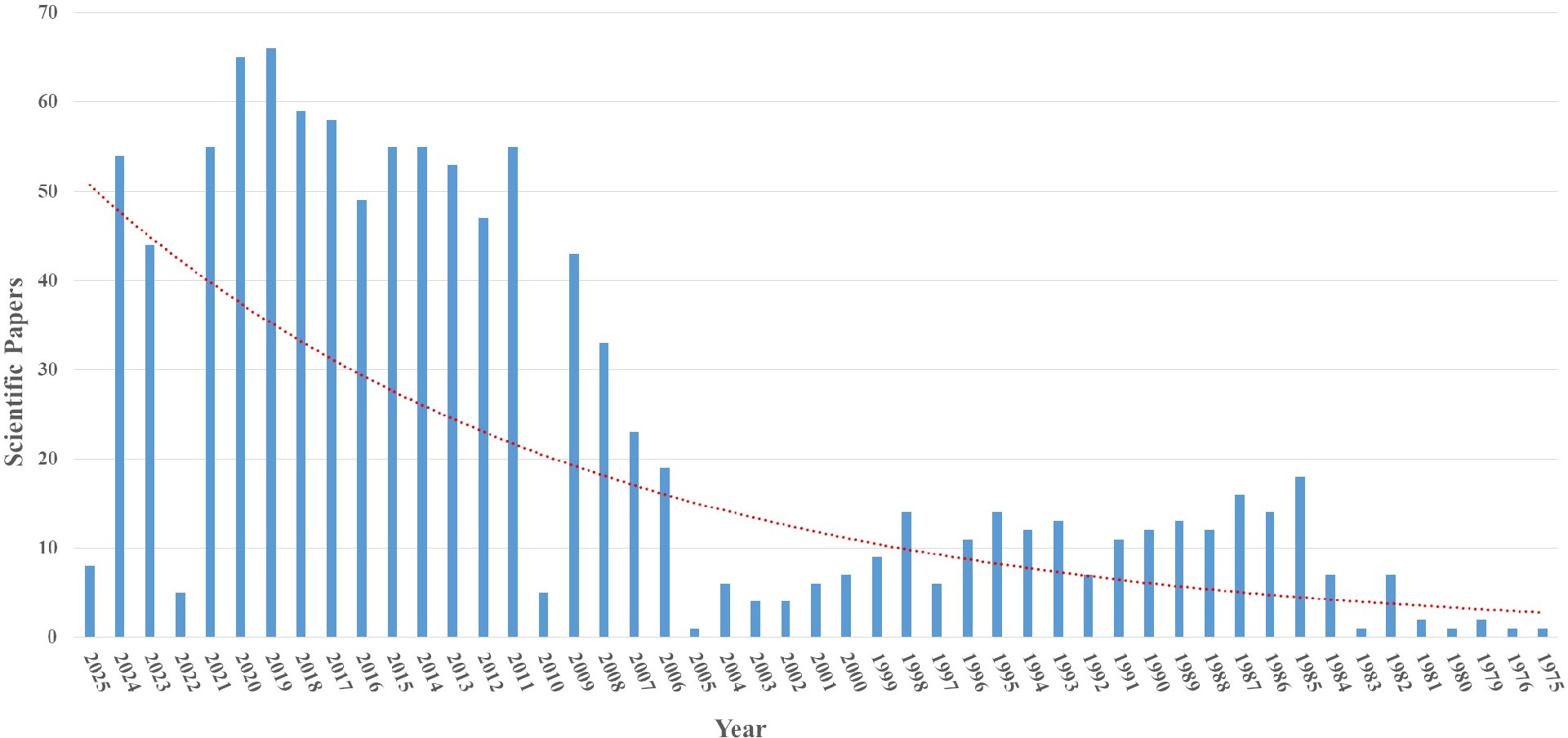
Seasonal influenza causes an estimated one billion infections, 3-5 million sever……
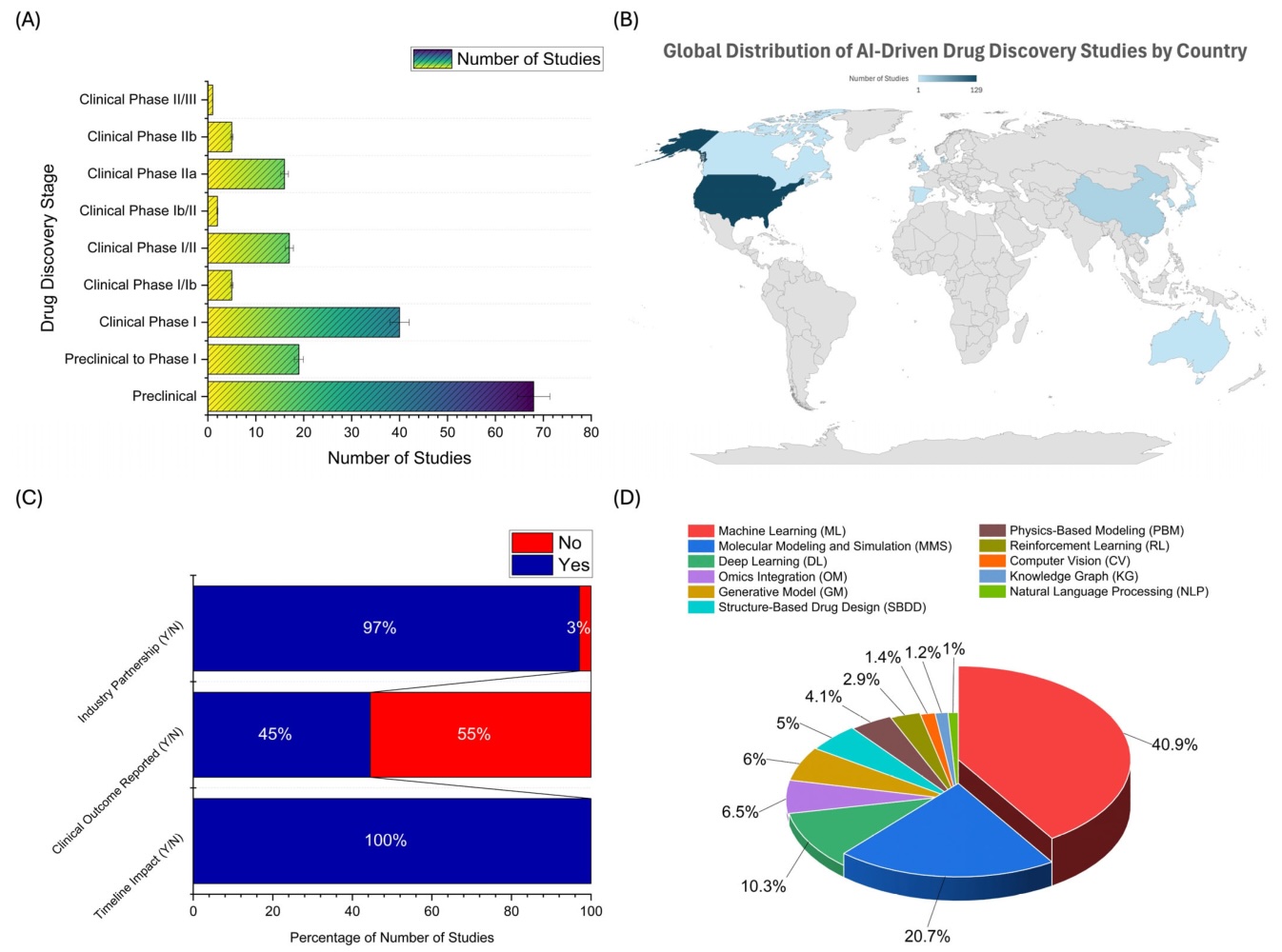
Artificial intelligence can now help researchers analyze antibody sequences, pre……
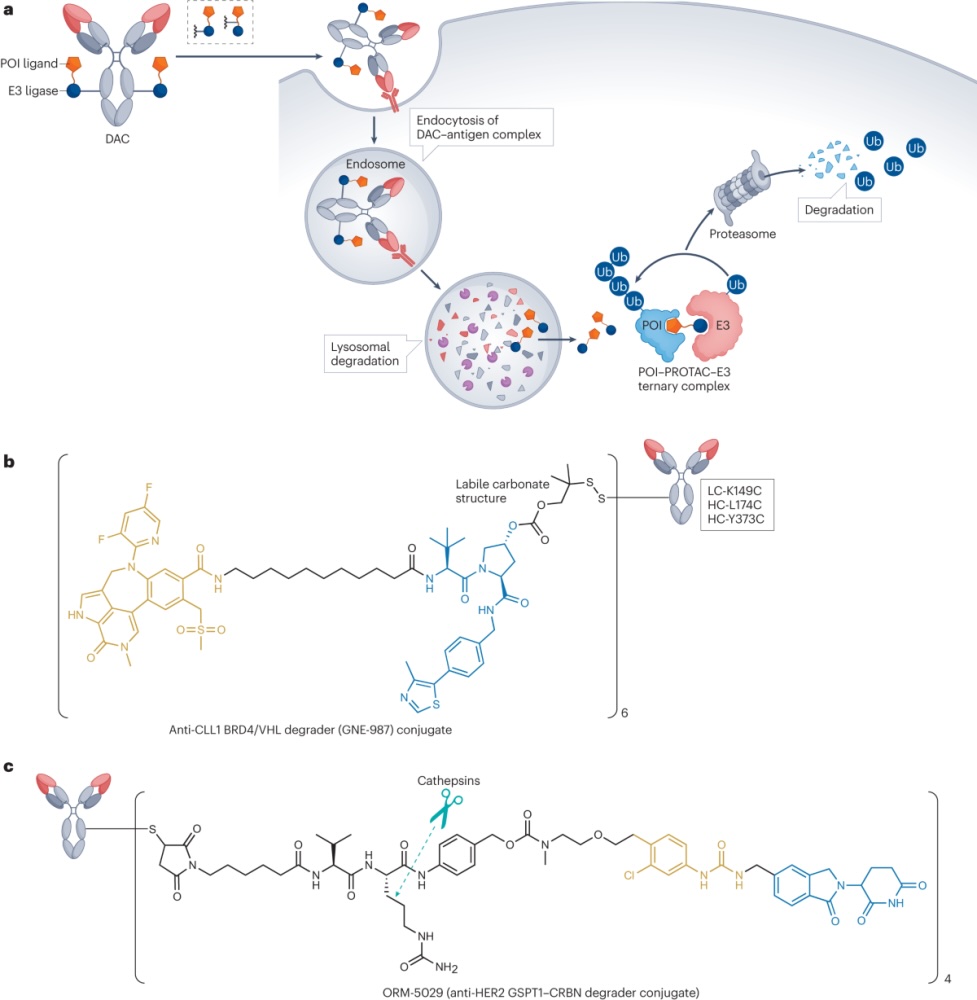
Degrader-antibody conjugates, or DACs, combine the targeting ability of antibodi……