The fight against Alzheimer’s disease (AD) has entered a new era, driven by major advances in immunotherapy. Monoclonal antibodies (mAbs) targeting hallmark proteins such as amyloid-beta (Aβ) and tau, have dominated recent research, clinical trials, and regulatory approvals. However, while new therapies show potential, the field faces critical questions about efficacy, safety, and scientific validity.
Traditional methods for generating antibodies against insoluble antigens like amyloid fibrils have relied heavily on animal immunization, often followed by humanization steps for therapeutic use. However, a recent study led by researchers from the University of Michigan introduces a new methodology using yeast surface display and fluorescence-activated cell sorting to isolate fully human, conformation-specific antibodies directly from nonimmune libraries.
This platform successfully produced antibodies against tau fibrils (associated with Alzheimer’s) and α-synuclein fibrils (linked to Parkinson’s) with high affinity and low off-target binding — rivaling or exceeding the specificity of clinical-stage antibodies such as zagotenemab and cinpanemab. This technological advancement could streamline therapeutic antibody development, reducing reliance on animal models and enabling quicker, more precise targeting of pathological aggregates.

While innovation in antibody design moves forward, real-world clinical results reveal more modest outcomes. A recent meta-analysis of phase III randomized controlled trials, led by researchers at Cleveland Clinic Lerner Research Institute, evaluated the cognitive outcomes and side effects of anti-Aβ mAbs in patients with Alzheimer’s.
Key findings:
Cognitive decline was slowed, but the effect size was small.
Safety concerns emerged, including amyloid-related imaging abnormalities (ARIA) like edema and hemorrhage, and increased rates of headache.
Early initiation of treatment (at the mild cognitive impairment stage) seemed more beneficial than later use.
Anti-amyloid therapies offer hope but deliver only modest clinical benefits. Importantly, they come with significant risks that clinicians must carefully weigh with patients and families.

Acknowledging the gap between clinical trial results and real-world effectiveness, researchers propose using target trial emulation frameworks to study newly approved therapies like lecanemab. This method leverages administrative healthcare data while minimizing biases inherent in observational studies. Key goals include assessing real-world safety and utilization of anti-Aβ mAbs, and informing clinicians, patients, and policymakers with more accurate post-approval data. As more mAbs enter clinical practice, real-world studies will be essential to truly understand their benefits and risks beyond the controlled environment of trials.

Beyond amyloid, researchers have turned attention to tau protein, another major pathological hallmark of AD. A systematic review of six randomized controlled trials evaluated the safety and efficacy of anti-tau monoclonal antibodies. They found that while reduction in tau levels in cerebrospinal fluid was achieved, no significant cognitive benefit (as measured by Clinical Dementia Rating Sum of Boxes, CDR-SB) was observed. However, anti-tau therapies appeared safe, with no increase in adverse event rates. Thus, simply clearing pathological proteins — whether amyloid or tau — does not necessarily translate into meaningful clinical improvement. Therapeutic targets may need to address broader mechanisms of neurodegeneration.
Finally, a growing concern questions whether reducing amyloid plaques alone should be sufficient grounds for drug approval. Current evidence suggests that plaque lowering does not consistently predict clinical benefit. Researchers now call for:
Stronger validation of surrogate biomarkers (imaging and fluid-based).
Exploration of new markers more closely tied to neurodegeneration and symptom progression.
Rigorous clinical endpoints in prevention trials, especially in asymptomatic populations.
Future drug development must prioritize clinical outcomes over biomarker changes, ensuring that therapies truly improve patient lives.

The Alzheimer’s therapeutic landscape is evolving rapidly, with new technologies promising faster, better antibody generation, while recent approvals offer patients new hope. Yet, caution is warranted: modest benefits, real-world risks, and scientific gaps urge a more careful, evidence-driven approach to therapy development and approval.
Biointron’s Q2 2026 Antibody Industry Trends report aims to explore the events a……
Seasonal influenza causes an estimated one billion infections, 3-5 million sever……
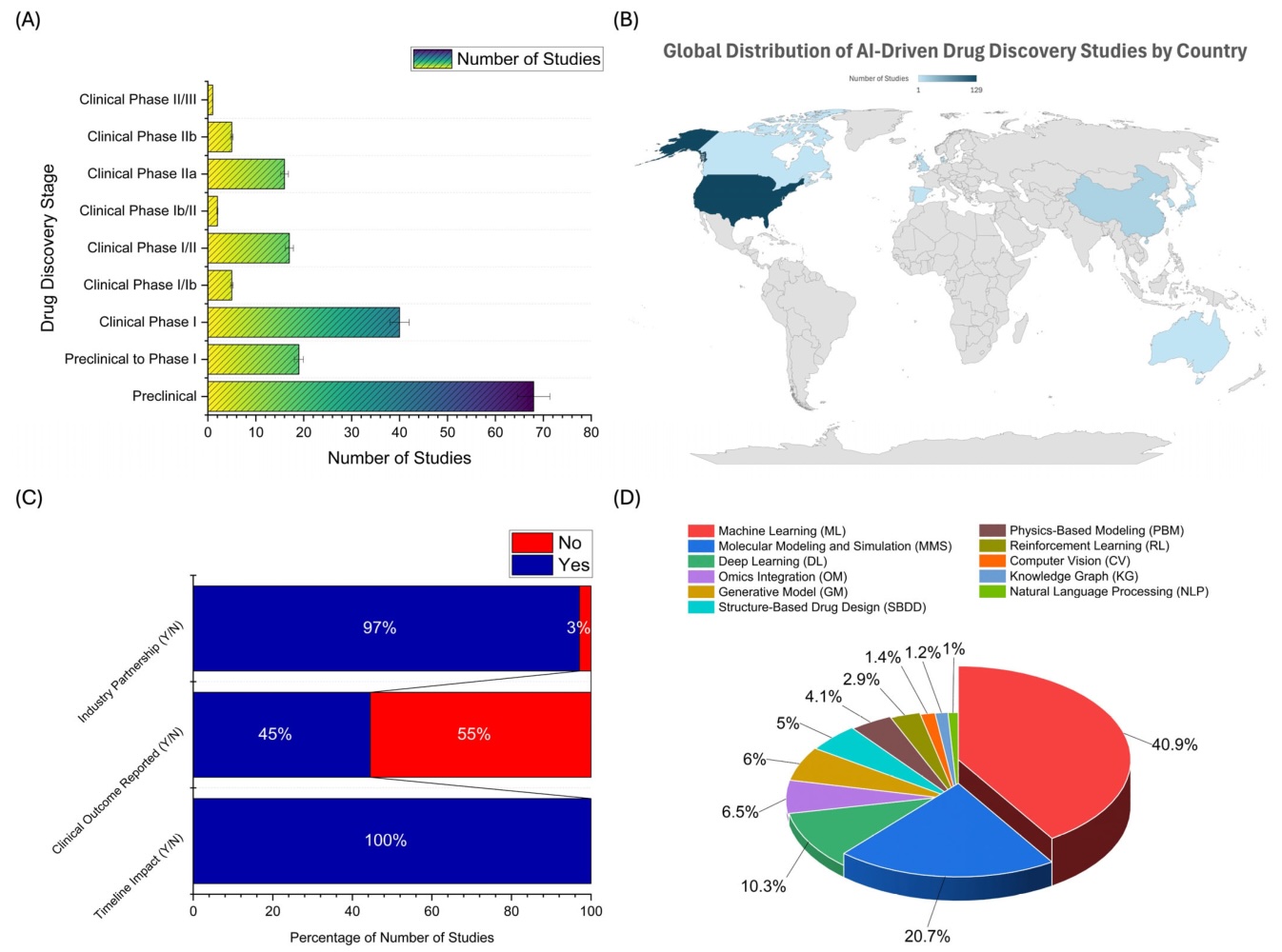
Artificial intelligence can now help researchers analyze antibody sequences, pre……
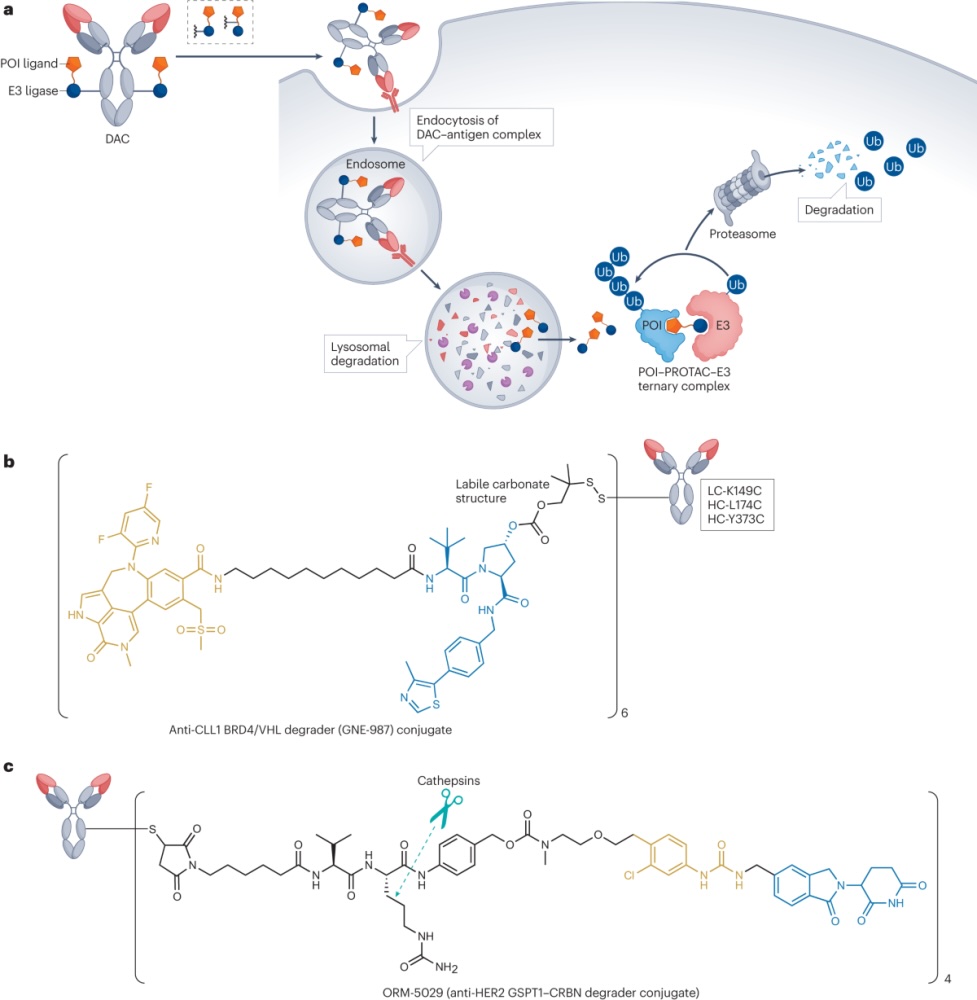
Degrader-antibody conjugates, or DACs, combine the targeting ability of antibodi……