A review by researchers from the University of Virginia highlights the role of antibody-dependent cellular phagocytosis (ADCP) in cancer immunotherapy. Unconjugated monoclonal antibodies (mAbs) have significantly impacted cancer treatment by targeting specific antigens on malignant cells. Widely used mAbs, such as anti-CD20 (rituximab, obinutuzumab), anti-HER2 (trastuzumab), and anti-CD38 (daratumumab), use ADCP to target and remove malignant cells. However, as monotherapies, these mAbs often produce insufficient cytotoxicity in vivo and are more effective in combination therapies. Additionally, the development of drug resistance presents a significant challenge.
Fc gamma receptors (FcγRs) are crucial for ADCP. These receptors, found on immune cells like macrophages, bind to the Fc portion of IgG antibodies. FcγRs are categorized into activating and inhibitory receptors, with their activation determined by the binding ratio of these receptors on the cell surface. The binding specificity and affinity for different IgG subclasses add complexity to this system. High affinity receptors are typically saturated with monomeric IgG, while low affinity receptors bind immune complexes during an immune response.
The activation of FcγR-mediated phagocytosis involves three steps: ligand-receptor binding, receptor clustering and phosphorylation, and actin-driven engulfment. This process results in the formation of a phagosome, which matures through fusion with endosomes and lysosomes, leading to target cell degradation. The phagosome's acidification enhances its degradative capacity, a process regulated by NADPH oxidase and other enzymes.
Complement ADCP
The complement system, an ancient immune surveillance system, plays a role in ADCP by opsonizing target cells with complement fragments such as C3b and iC3b. Complement receptors (CRs) on immune cells recognize these fragments, promoting phagocytosis. CR3 is considered a key mediator of complement-mediated phagocytosis due to its high affinity for iC3b. Complement activation involves three pathways—classical, lectin, and alternative—all converging at the formation of a C3 convertase.
Synergy Between Complement and FcγR ADCP
Crosstalk between FcγRs and CRs enhances the phagocytosis of targets opsonized with both IgG and complement fragments. This synergy was first noted in autoimmune hemolytic anemia models, where complement activation increased the clearance of IgG-opsonized red blood cells (RBCs). Studies have shown that combined opsonization with IgG and C3b results in higher phagocytosis rates and inflammatory cytokine production by neutrophils.
ADCP in Treatment of Human Malignancies
Therapeutic mAbs can induce cytotoxicity through various mechanisms, including ADCP. Rituximab, a prototypic anti-CD20 mAb, effectively treats B-cell malignancies by inducing ADCP. However, its monotherapy efficacy is limited, often requiring combination with chemotherapy or other targeted therapies. For example, combining rituximab with chemotherapy or targeted drugs like Bruton tyrosine kinase (BTK) inhibitors has shown improved clinical outcomes in chronic lymphocytic leukemia (CLL).
Mechanistic Insights from Mouse Models
Mouse models have provided valuable insights into the mechanisms of ADCP. Studies have shown that fixed macrophages in the liver and spleen play a significant role in clearing circulating B cells via ADCP. The efficacy of anti-CD20 mAbs depends on the activation of FcγRs on macrophages. Kupffer cells in the liver have been identified as crucial effectors in clearing B cells from circulation following anti-CD20 mAb treatment.
Several factors limit the efficacy of ADCP in vivo:
Inhibitory Receptors: FcγRIIb, the sole inhibitory FcγR, dampens FcγR-mediated phagocytosis by recruiting phosphatases that dephosphorylate key signaling molecules. The balance between activating and inhibitory signals on phagocytes determines the ADCP threshold.
Complement Limitations: Cancer patients often exhibit deficiencies in complement proteins, and therapeutic mAbs can lead to complement consumption, reducing their efficacy. Complement consumption has been observed in CLL patients treated with rituximab, resulting in reduced cytotoxic activity.
CD47 as a Negative Regulator: CD47 on cancer cells interacts with SIRPα on macrophages, sending a "don't eat me" signal that inhibits phagocytosis. High CD47 expression is associated with poor mAb efficacy. Blocking the CD47-SIRPα axis has shown promise in enhancing mAb-induced phagocytosis in various cancers.
Phagocytic Exhaustion: Macrophages can become "exhausted" after extensive phagocytosis, losing their ability to engulf additional targets. This exhaustion is associated with the downregulation of FcγRs on the macrophage surface. Strategies to overcome phagocytic exhaustion could enhance the therapeutic efficacy of mAbs.
Loss of Target Antigen: Malignant cells can downregulate or shed target antigens, reducing their susceptibility to mAb-induced cytotoxicity. Trogocytosis, where immune complexes are removed from target cells without engulfment, contributes to this resistance mechanism.
Pharmacokinetics: The large size of mAbs limits their penetration into tissues, affecting their ability to reach and clear target cells. Enhanced tissue penetration strategies are needed to improve mAb efficacy.
Effector to Target Ratios: The ratio of effector cells (e.g., macrophages) to target cells can influence the effectiveness of ADCP. High tumor cell burdens can overwhelm the available effector cells, reducing mAb efficacy. Modulating the cytotoxic activity of individual macrophages may improve clearance of malignant cells.
Immune Modulation by ADCP: FcγR activation can induce a proinflammatory environment, but the role of FcγR-dependent ADCP in modulating macrophage responses remains understudied. ADCP can lead to the release of anti-inflammatory cytokines, potentially impairing adaptive immune responses. Uncoupling cytokine release from ADCP could enhance mAb therapeutic benefit.
Several approaches are being explored to enhance ADCP efficacy:
Antibody Engineering: Fc engineering can modify mAbs to improve their affinity for FcγRs or complement activation. Fc-defucosylation increases FcR affinity, enhancing phagocytosis. Fc mutations that promote hexamerization of antigen-ligated mAbs can boost complement activation and phagocytosis.
Targeting Inhibitory Pathways: Blocking the CD47-SIRPα axis can synergize with mAb therapies, improving clinical outcomes. Several anti-CD47 and anti-SIRPα mAbs are currently in clinical trials, showing promise in enhancing ADCP and overall mAb efficacy.
Novel Therapeutic Regimens: Combining mAbs with innate immune checkpoint inhibitors like anti-CD47 antibodies has shown improved responses in lymphoma. Optimizing mAb dosing regimens to avoid prolonged inhibition of innate immune cytotoxicity and antigen loss could enhance therapeutic efficacy.
In conclusion, ADCP represents a powerful mechanism for mAb-induced cytotoxicity in cancer immunotherapy. Understanding the factors limiting ADCP efficacy and developing strategies to overcome these barriers will enhance the therapeutic potential of mAbs in treating malignancies.
References:
Van Wagoner, C. M., Rivera-Escalera, F., Jaimes-Delgadillo, N. C., Chu, C. C., Zent, C. S., & Elliott, M. R. (2023). Antibody-mediated phagocytosis in cancer immunotherapy. Immunological Reviews, 319(1), 128-141. https://onlinelibrary.wiley.com/doi/10.1111/imr.13265
For an antibody candidate, strong target binding is only part of the path toward……
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
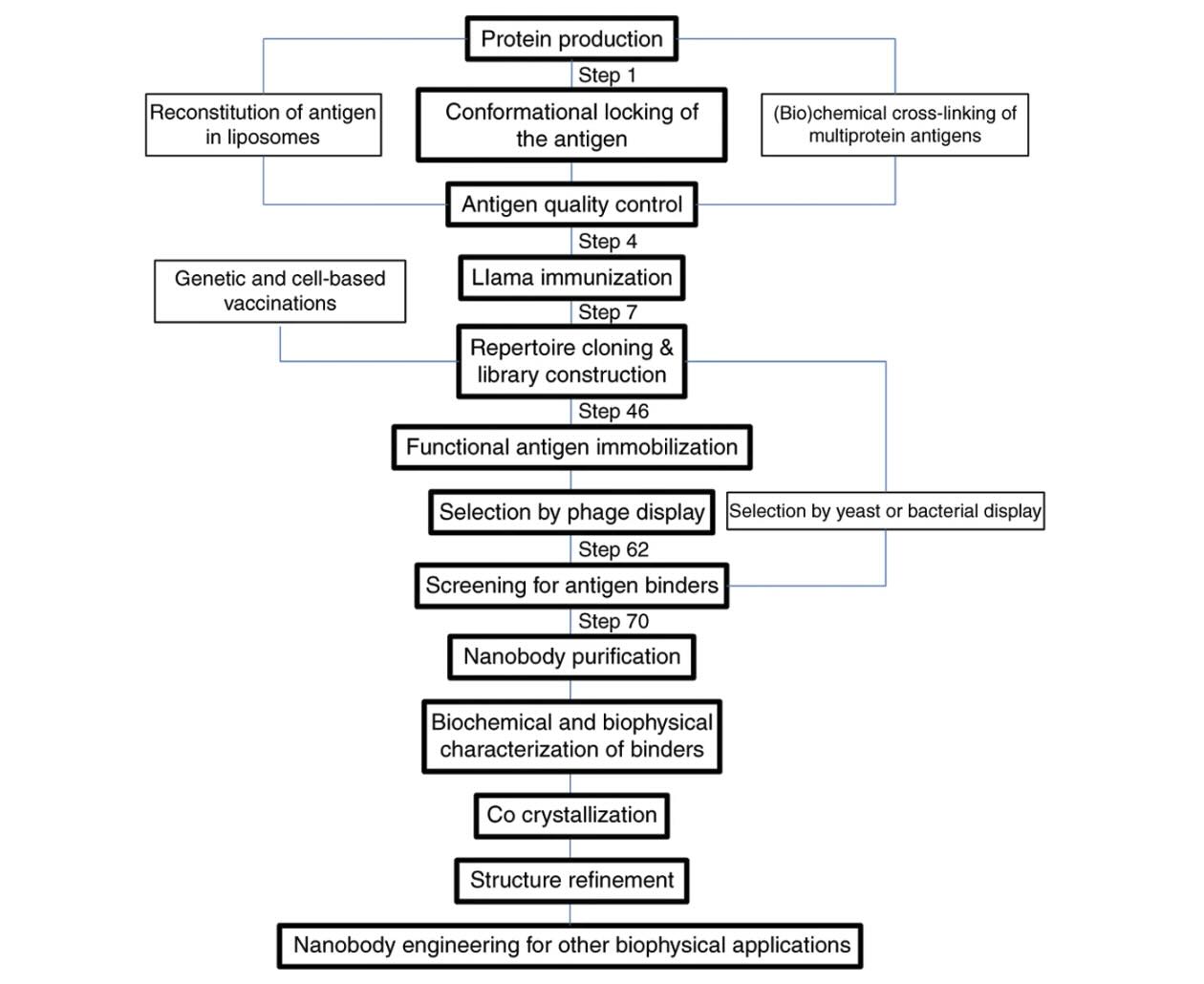
Explore how VHH antibodies stabilize protein conformations for crystallography, ……