Cancer immunotherapy has emerged as a transformative approach in oncology, with immune checkpoint inhibitors (ICIs) at the forefront. ICIs work by blocking regulatory pathways in T cells that cancer cells exploit to evade immune detection.
Immune checkpoints are regulatory pathways that maintain self-tolerance and modulate the duration and amplitude of physiological immune responses. The most well-studied checkpoints are cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed death-1 (PD-1), along with its ligand PD-L1. Tumor cells often exploit these pathways to avoid immune surveillance.
CTLA-4 is expressed on T cells and acts as a negative regulator of T cell activation. Ipilimumab, a monoclonal antibody against CTLA-4, was the first ICI approved by the FDA for the treatment of metastatic melanoma. By blocking CTLA-4, ipilimumab enhances T cell activation and proliferation, thereby augmenting anti-tumor immunity.
PD-1 is expressed on the surface of T cells, and its interaction with PD-L1, expressed on tumor cells, leads to the inhibition of T cell activity. Monoclonal antibodies such as pembrolizumab and nivolumab target PD-1, while atezolizumab targets PD-L1, preventing this interaction and restoring T cell function.
ICIs have demonstrated remarkable efficacy across a variety of malignancies, including melanoma, non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), and Hodgkin lymphoma. The clinical success of ICIs has led to their rapid adoption and integration into standard cancer treatment protocols.
The use of ipilimumab in melanoma was a pivotal moment in cancer therapy, showing improved overall survival in patients with advanced disease. Subsequent studies with PD-1 inhibitors further extended survival benefits, establishing ICIs as the standard of care in melanoma.
ICIs have shown significant efficacy in non-small cell lung cancer (NSCLC), particularly in patients with high PD-L1 expression. Pembrolizumab, in combination with chemotherapy, has become a first-line treatment for metastatic NSCLC, demonstrating substantial improvements in survival outcomes.
In renal cell carcinoma (RCC), nivolumab has shown improved overall survival compared to everolimus in previously treated patients. The combination of nivolumab and ipilimumab has also been approved for first-line treatment, highlighting the potential of combination ICI therapy.
Antibody-drug conjugates (ADCs) combine the specificity of monoclonal antibodies with the cytotoxic potential of chemotherapy, offering targeted delivery of therapeutic agents. Combining ADCs with ICIs can potentiate anti-tumor immunity by not only directly killing tumor cells but also enhancing immune recognition and response.
Bispecific antibodies are engineered to simultaneously bind two different antigens, which can redirect immune cells to tumor cells. The combination of bispecific antibodies with ICIs can enhance the recruitment and activation of T cells at the tumor site, providing a multifaceted approach to cancer therapy.
One of the major challenges with ICIs is the management of immune-related adverse events (irAEs), which can affect any organ system and vary in severity. Understanding the mechanisms underlying irAEs and developing strategies to mitigate them is crucial for the broader application of ICIs.
Identifying biomarkers that predict response to ICIs is essential for optimizing patient selection and treatment outcomes. PD-L1 expression, tumor mutational burden (TMB), and microsatellite instability (MSI) are currently being investigated as potential biomarkers.
The future of ICIs lies in their integration with other therapeutic modalities, including targeted therapies, radiation, and other immunotherapies. Preclinical and clinical studies are ongoing to identify the most effective combinations and treatment sequences.
Immune checkpoint inhibitors represent a significant advancement in cancer therapy, offering new hope for patients with previously untreatable malignancies. Their integration with antibody therapeutics presents a promising frontier, combining the strengths of both approaches to enhance anti-tumor efficacy. Ongoing research and clinical trials will continue to refine these therapies, aiming to maximize their benefits while minimizing adverse effects.
Shiravand, Y., Khodadadi, F., Amin Kashani, S. M., Hosseini-Fard, S. R., Hosseini, S., Sadeghirad, H., Ladwa, R., & Kulasinghe, A. (2022). Immune Checkpoint Inhibitors in Cancer Therapy. Current Oncology, 29(5), 3044-3060. https://www.mdpi.com/1718-7729/29/5/247
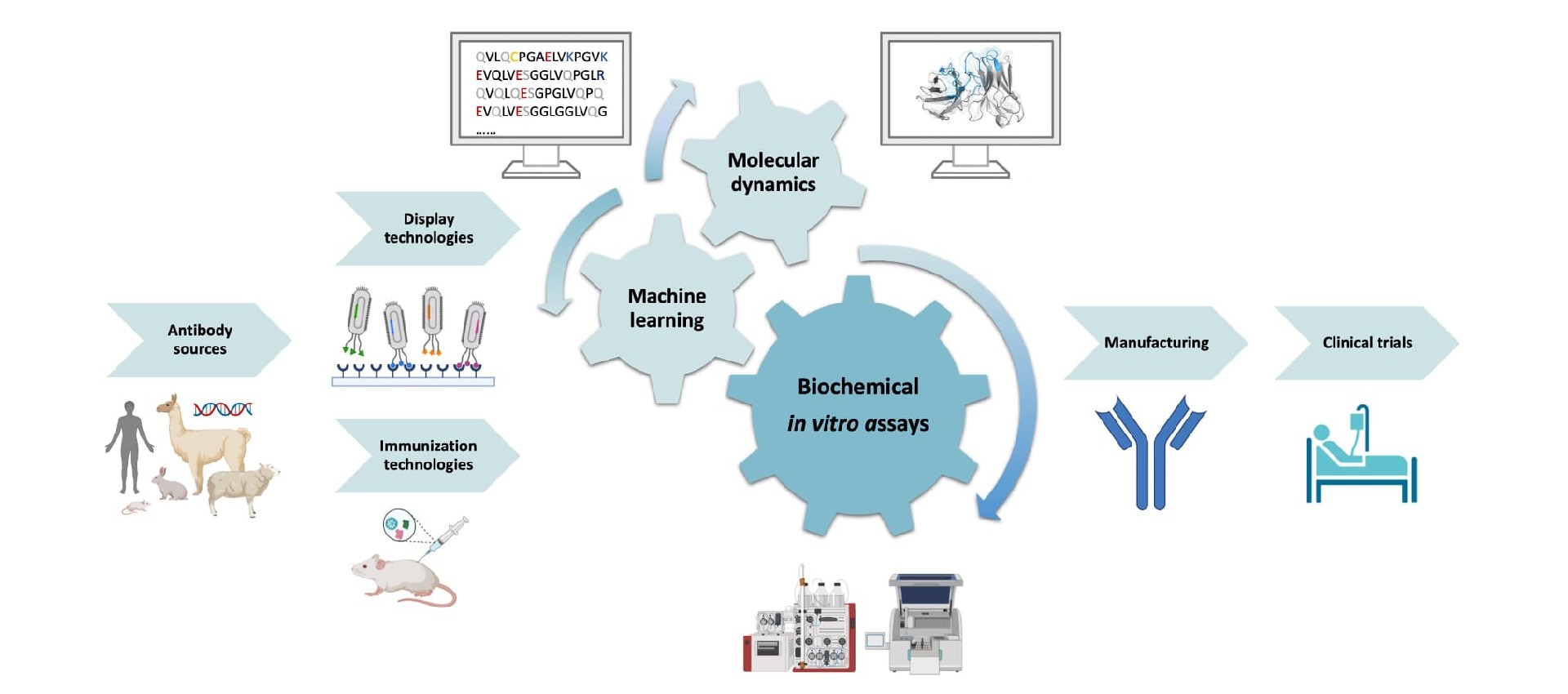
For an antibody candidate, strong target binding is only part of the path toward……
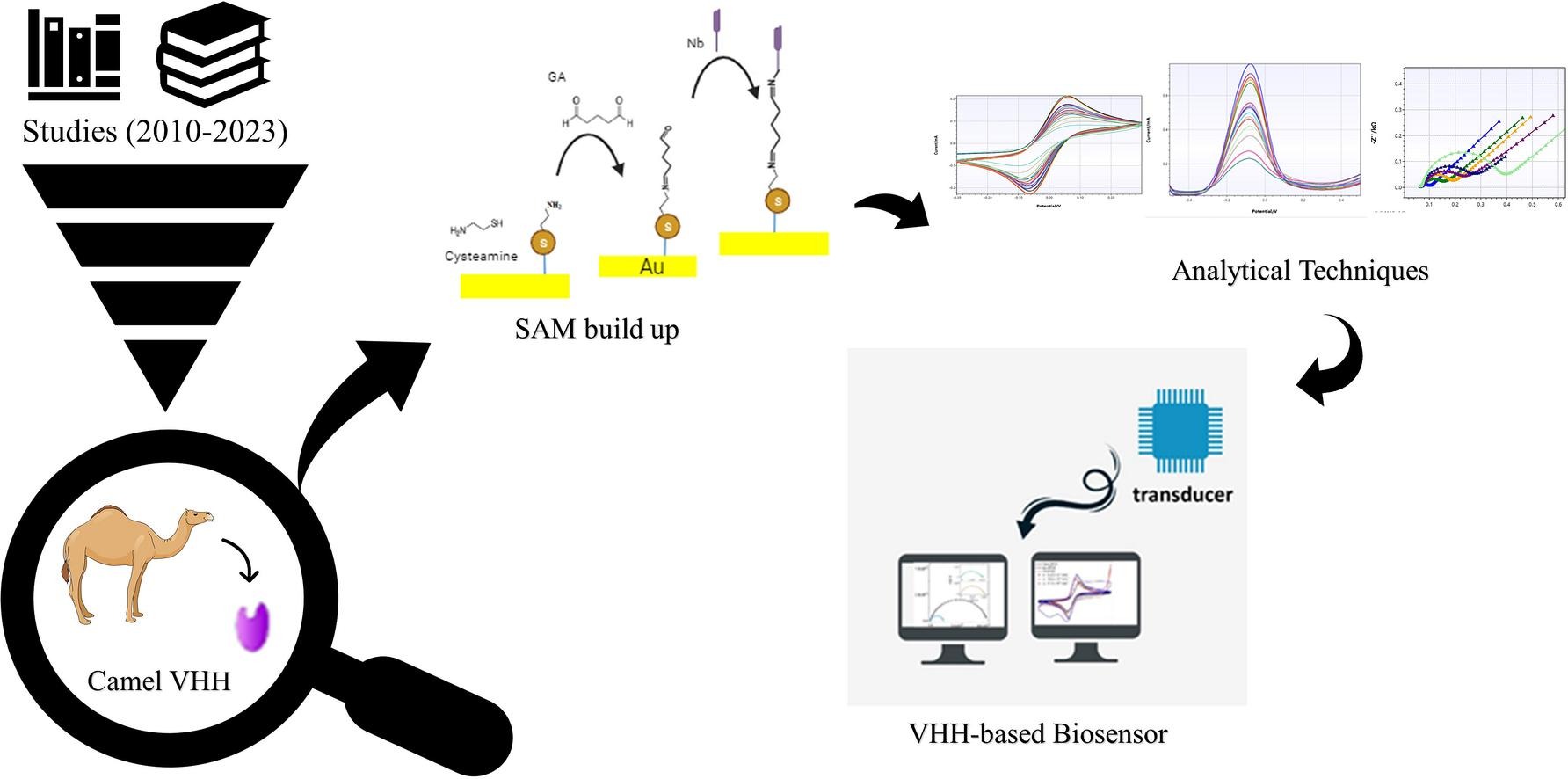
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
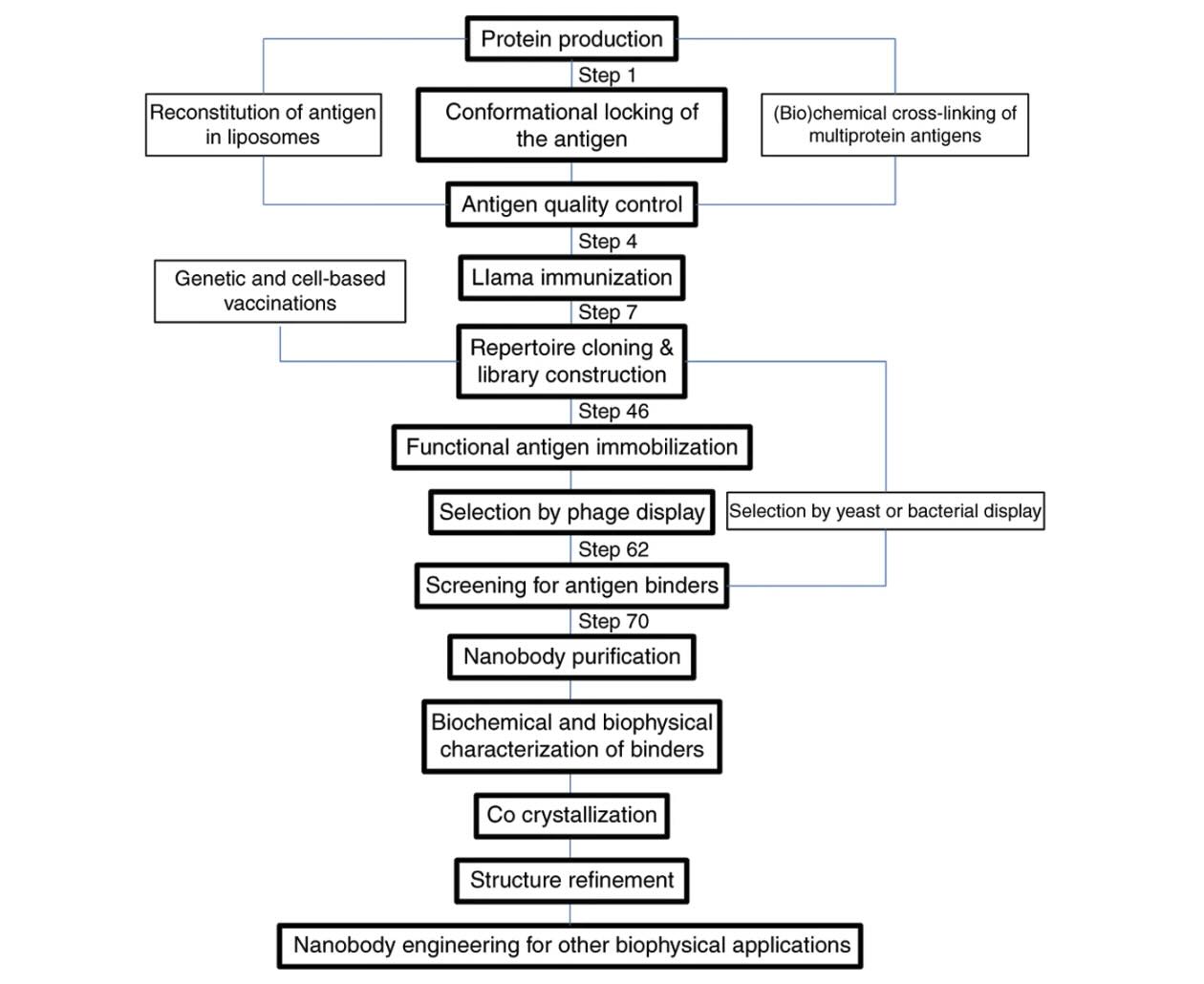
Explore how VHH antibodies stabilize protein conformations for crystallography, ……