Pembrolizumab (sold as Keytruda) is a humanized monoclonal antibody targeting programmed cell death protein 1 (PD-1), a key immune checkpoint receptor that modulates T-cell activity. As an immune checkpoint inhibitor, pembrolizumab prevents tumor cells from evading immune detection by blocking the PD-1 receptor, thereby enhancing the anti-tumor immune response.
Traditionally, cancer therapies have been approved based on the anatomical site of the tumor (e.g., lung cancer, breast cancer). However, in 2017, pembrolizumab became the first drug granted FDA approval based on a tumor’s molecular characteristics rather than its tissue of origin. Specifically, this approval applied to tumors exhibiting high microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR), marking a major shift toward biomarker-driven precision oncology.1
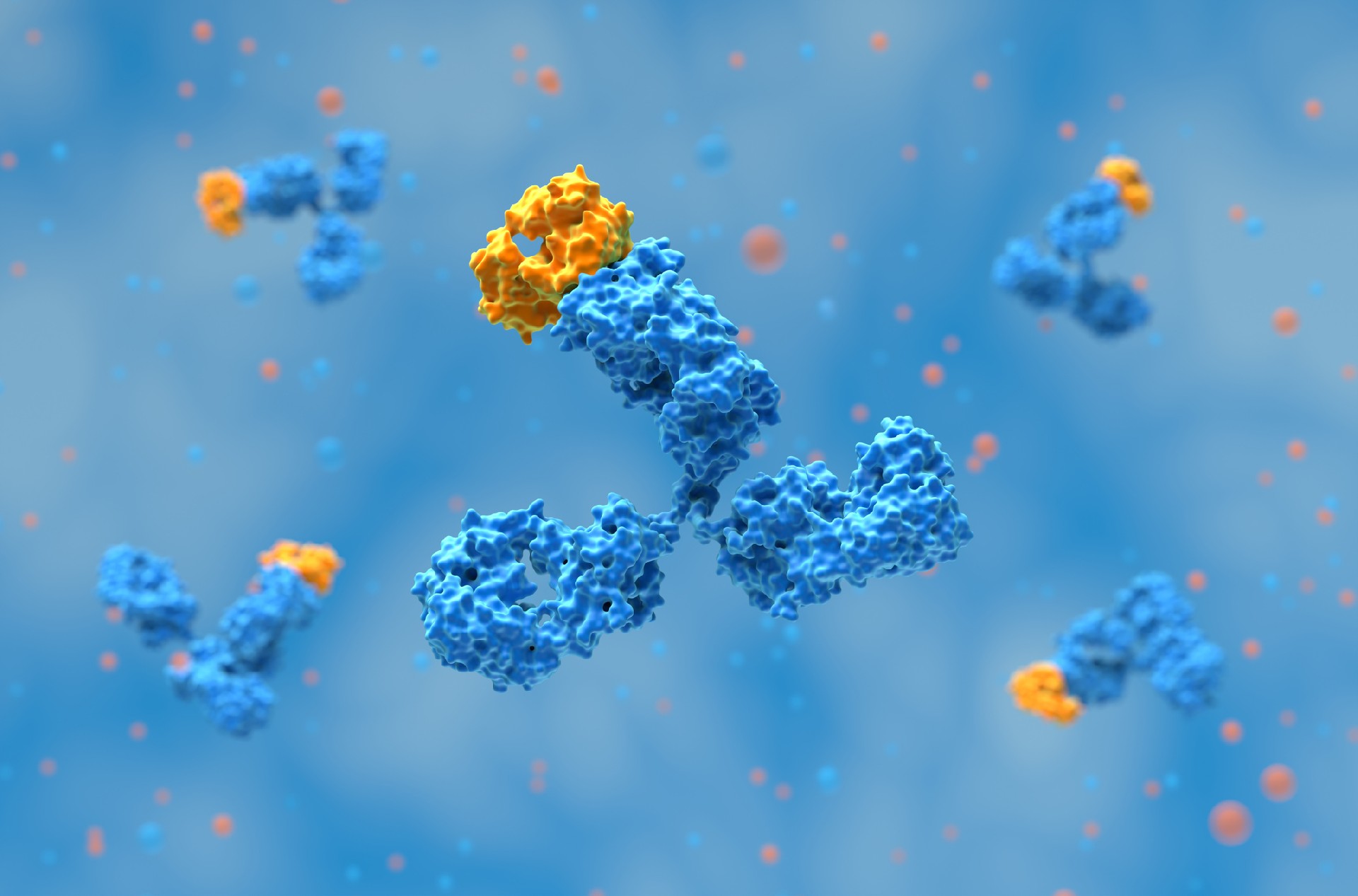
PD-1 is an inhibitory receptor expressed on activated T cells. It interacts with its ligands, PD-L1 and PD-L2, to downregulate immune responses, preventing excessive inflammation and autoimmunity. Tumor cells exploit this pathway by upregulating PD-L1, effectively “turning off” T cells and escaping immune destruction.
Pembrolizumab binds PD-1 and blocks its interaction with PD-L1 and PD-L2, preventing immune suppression. This allows cytotoxic T cells to recognize and attack tumor cells more effectively. The therapeutic efficacy of pembrolizumab has been demonstrated across various malignancies, particularly in tumors with high mutational burdens that generate neoantigens capable of triggering a strong immune response.

On May 23, 2017, the FDA approved pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H/dMMR solid tumors that had progressed following prior therapy. This decision was based on data from multiple clinical trials demonstrating high response rates in MSI-H/dMMR tumors, regardless of their tissue of origin.
This approval was notable for several reasons:
First tissue-agnostic approval: Pembrolizumab became the first cancer drug approved based solely on a genetic biomarker rather than tumor location.
Regulatory precedent: The decision established a new framework for future approvals of biomarker-driven therapies.
Clinical impact: It provided a new treatment option for patients with MSI-H/dMMR cancers, many of whom had limited therapeutic alternatives.
The FDA approval was supported by data from five clinical trials involving 149 patients with MSI-H/dMMR tumors across 15 cancer types. The objective response rate (ORR) was 39.6%, with 78% of responding patients maintaining their response for at least six months. The strongest responses were observed in colorectal, endometrial, and gastric cancers.2
Related: Bispecific Antibodies in Cancer Therapy: Engineering, Mechanisms, and Clinical Applications
Mismatch repair deficiency results from mutations in genes responsible for correcting errors during DNA replication, leading to microsatellite instability—a condition characterized by widespread mutations. MSI-H/dMMR status is most commonly associated with:
Colorectal cancer: About 15% of cases are MSI-H, with 5% being hereditary (Lynch syndrome).
Endometrial cancer: MSI-H is observed in up to 30% of cases.
Gastric cancer: Approximately 10–20% of cases exhibit MSI-H.
Other cancers, including pancreatic, biliary tract, and prostate cancer, can also display MSI-H features, albeit at lower frequencies. Tumors with MSI-H/dMMR status tend to have high mutational burdens, increasing their susceptibility to immune checkpoint blockade.
DNA mismatch repair deficiency (MMRd) occurs when cells lose the ability to correct errors made during DNA replication. Normally, the mismatch repair system identifies and fixes these errors to maintain genomic stability. When this system fails, uncorrected mutations accumulate, increasing the risk of malignant transformation. High microsatellite instability (MSI-H) is a direct consequence of MMRd, characterized by alterations in the length of microsatellites—short, repetitive DNA sequences—due to defective repair mechanisms. MSI-H tumors exhibit a high mutational burden, which can generate neoantigens that make them more susceptible to immune checkpoint inhibitors like pembrolizumab.3

Traditionally, cancer treatments have been categorized and approved based on tumor histology and tissue of origin. Pembrolizumab’s approval based on a biomarker rather than tumor location represents a shift toward precision oncology. This approach enables the identification of patients most likely to benefit from immunotherapy, irrespective of their cancer type.
Increased treatment options: Patients with rare or difficult-to-treat cancers that express MSI-H/dMMR can now receive pembrolizumab.
More efficient drug development: Instead of conducting separate trials for each cancer type, a single biomarker-driven trial can evaluate efficacy across multiple malignancies.
Higher response rates in selected patients: The ORR of pembrolizumab in MSI-H/dMMR tumors was significantly higher than in unselected populations.
Pembrolizumab’s success paved the way for additional tissue-agnostic approvals. In 2018, the FDA granted a similar approval for the TRK inhibitor larotrectinib in tumors with NTRK gene fusions. This trend underscores the growing emphasis on genetic and molecular markers over histological classifications in oncology.
Related: Large-Scale Antibody Production
Pembrolizumab’s development and approval process highlighted several key trends in monoclonal antibody therapeutics:
Checkpoint inhibitors as a major class of biologics: The success of pembrolizumab reinforced the therapeutic potential of PD-1/PD-L1 blockade, leading to the development of additional checkpoint inhibitors, including nivolumab (Opdivo) and atezolizumab (Tecentriq).
The importance of biomarker selection: The use of MSI-H/dMMR as a predictive biomarker demonstrated the value of identifying patient subgroups most likely to respond to therapy.
Accelerated regulatory pathways: Pembrolizumab received FDA breakthrough therapy designation, expediting its development and approval. This approach is now widely used for promising biologic therapies.
The field of immuno-oncology continues to evolve, with new strategies aimed at overcoming resistance and improving response rates:
Combination therapies: Pembrolizumab is being tested in combination with other immunotherapies, chemotherapy, and targeted agents to enhance efficacy.
Next-generation checkpoint inhibitors: Research is ongoing into alternative immune checkpoints such as LAG-3 and TIGIT, which may complement PD-1 blockade.
Personalized immunotherapy approaches: Advances in tumor profiling and AI-driven biomarker discovery are improving patient selection for immunotherapy.
Pembrolizumab’s tissue-agnostic approval established a model that could be applied to other biomarker-driven therapies. Potential future targets include:
Tumor mutational burden (TMB): High TMB tumors may respond similarly to checkpoint inhibitors, regardless of histology.
DNA repair deficiency markers: Beyond MSI-H/dMMR, other DNA repair defects, such as BRCA mutations, may predict immunotherapy response.
Epigenetic and transcriptomic markers: Emerging research is identifying additional molecular features that could define immunotherapy-responsive cancers.
Pembrolizumab’s approval for MSI-H/dMMR tumors marked a significant milestone in oncology, demonstrating the potential of antibody-based therapies in biomarker-driven treatment paradigms. As research continues, tissue-agnostic approvals will likely become more common, further advancing the field of precision immunotherapy.
Related: How Antibodies are Used in Cancer Immunotherapy

At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including HTP Recombinant Antibody Production, Bispecific Antibody Production, Large Scale Antibody Production, and Afucosylated Antibody Expression.
Mass production of proteins is frequently influenced by factors such as cost, turnaround time, and regulatory compliance, and is subject to stringent quality control and assurance measures. Biointron has been dedicated to delivering high-quality products to biotechnology and pharmaceutical customers worldwide. In order to meet our customers' needs for gram-scale proteins, with over 10 years of expertise in protein production, Biointron has established a mass protein production service with validated cell culture technology, which allows rapid and large amounts of recombinant proteins production. This service offers scaled-up production of recombinant antibodies or proteins from milligram to gram levels in weeks. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Geantă, M., & Cioroboiu, C. (2017). The FDA Changed Everything. Biomedicine Hub, 2(Suppl 1), 52. https://doi.org/10.1159/000481614
Shaywitz, D. (2017, July 26). The Startling History Behind Merck’s New Cancer Blockbuster. Forbes. https://www.forbes.com/sites/davidshaywitz/2017/07/26/the-startling-history-behind-mercks-new-cancer-blockbuster/
Flynn JP, Gerriets V. Pembrolizumab. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546616/
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……