Polyclonal antibodies (pAbs) represent one of the earliest forms of antibody therapeutics, with clinical use dating back to serum therapies for infectious diseases such as diphtheria and tetanus in the late 19th century. These preparations, derived from immunized animals or human donors, consist of heterogeneous antibody populations capable of recognizing multiple epitopes on a target antigen. This multiepitope binding distinguishes pAbs from monoclonal antibodies (mAbs), which are highly specific to a single epitope.
Despite their early dominance, pAbs have been largely displaced by mAbs since the early 2000s due to advances in hybridoma technology, transgenic animal platforms, and single B-cell cloning methods. Currently, over 140 mAbs are approved in the United States compared to approximately 40 pAb therapies. However, the past five years have seen renewed interest in pAbs, driven by their ability to address biological complexity that single-epitope targeting cannot adequately resolve.1
This shift is particularly relevant in contexts such as rapidly mutating pathogens, complex autoimmune conditions, and heterogeneous tumor microenvironments, where antigenic variability can compromise monoclonal efficacy.
The current clinical landscape demonstrates that pAbs remain essential in several therapeutic areas. These include immune globulin therapies, anti-thymocyte globulin (ATG), antivenoms, and convalescent plasma-based treatments.
Immune globulin products, particularly intravenous immunoglobulin (IVIG), are widely used for primary immunodeficiency disorders and autoimmune diseases. These products are derived from pooled plasma of thousands of donors, providing a highly diverse antibody repertoire. Their mechanisms include immunomodulation and neutralization of pathogenic autoantibodies, although these mechanisms are not fully defined.
In infectious disease settings, pAbs provide passive immunity through broad antigen recognition. Convalescent plasma therapy (CPT), for example, has been used historically and during the COVID-19 pandemic. Monoclonal antibodies have had improvements in cross-neutralization and synergistic use with antibiotics, and typically demonstrate higher and more consistent efficacy in some cases, but pAbs retain advantages in addressing viral variants due to their poly-specificity.
However, the clinical and commercial positioning of antibody-based therapies for infectious diseases is shaped by competition with lower-cost interventions such as antibiotics, small molecules, and vaccines. Their impact in infectious diseases has been more limited than in chronic conditions, due to prioritization of vaccines for endemic diseases, relatively small and specialized markets, and the high cost of goods associated with antibody cocktails required to prevent antigenic escape. In this context, polyclonal hyperimmune immunoglobulins remain a cost-effective alternative, particularly when derived from vaccinated or convalescent populations using standardized and scalable purification methods.2

Anti-thymocyte globulin represents another established application, particularly in transplantation and aplastic anemia. These pAbs target T cells for depletion, enabling immunosuppression and improved transplant outcomes. Their continued use reflects both efficacy and cost-effectiveness in specific clinical scenarios.
Antivenoms further illustrate the importance of pAbs in targeting complex toxin mixtures. The ability to neutralize multiple venom components simultaneously remains difficult to replicate with monoclonal approaches, although recombinant alternatives are under development.
Traditional pAb production relies on immunization of animals or collection of human plasma, followed by fractionation, purification, and viral inactivation steps. Production includes antigen exposure, plasma or serum collection, chromatographic purification, and final formulation into therapeutic products.
This approach introduces several challenges:
Batch-to-batch variability, due to biological heterogeneity in donor responses
Limited scalability, particularly for plasma-derived products
Supply constraints, driven by donor availability
Immunogenicity risks, especially with animal-derived antibodies
These limitations have historically favored the adoption of mAbs, which offer higher consistency and defined molecular composition.

Recent technological developments are redefining the boundaries between monoclonal and polyclonal modalities. Recombinant polyclonal antibodies (RpAbs) represent a key innovation, combining the diversity of pAbs with the consistency of recombinant expression systems.
RpAbs are generated by isolating B cells from immunized or convalescent donors, capturing paired heavy and light chain sequences, and expressing these as large antibody libraries in mammalian systems such as CHO cells. The process enables controlled production of hundreds to thousands of defined antibody clones within a single batch.
In parallel, transgenic animal technologies are being developed to produce human or humanized pAbs. Transchromosomic bovines, for example, carry human immunoglobulin loci and can generate fully human antibodies following immunization.
Similarly, glyco-humanized pAbs derived from genetically modified pigs lacking key glycosylation enzymes demonstrate reduced immunogenicity and improved safety profiles. These platforms are being evaluated in infectious disease and oncology applications, with several candidates progressing through clinical trials.
High-throughput Fully Human Antibody Discovery Platform →
Monoclonal antibodies continue to dominate the therapeutic antibody market due to their specificity, reproducibility, and decreasing manufacturing costs. They are particularly effective in oncology and targeted immunotherapy applications.
However, pAbs maintain advantages in scenarios requiring:
Broad epitope coverage
Reduced susceptibility to antigen escape
Rapid response to emerging pathogens
Recombinant polyclonal systems, transgenic production platforms, and engineered antibody cocktails are expected to expand the therapeutic scope of antibody-based interventions.3 However, regulatory requirements, cost considerations, and manufacturing complexity will influence the pace of adoption.
For applications involving antigenic diversity and rapid evolution, pAbs and their next-generation derivatives are likely to remain essential components of the therapeutic antibody landscape.
Wightman, P., & Kelton, W. (2025). Recent developments and future clinical prospects of polyclonal antibody therapies. Expert Opinion on Biological Therapy, 25(12), 1285–1298. https://doi.org/10.1080/14712598.2025.2606053
Berry, J. D., & Gaudet, R. G. (2011). Antibodies in infectious diseases: Polyclonals, monoclonals and niche biotechnology. New Biotechnology, 28(5), 489. https://doi.org/10.1016/j.nbt.2011.03.018
Ferrara, F., Gaiotto, T., Naranjo, L., Tian, H., Gräslund, S., Dobrovetsky, E., Hraber, P., Lund-Johansen, F., Saragozza, S., Sblattero, D., Kiss, C., & Bradbury, A. R. (2014). Recombinant renewable polyclonal antibodies. MAbs, 7(1), 32. https://doi.org/10.4161/19420862.2015.989047
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
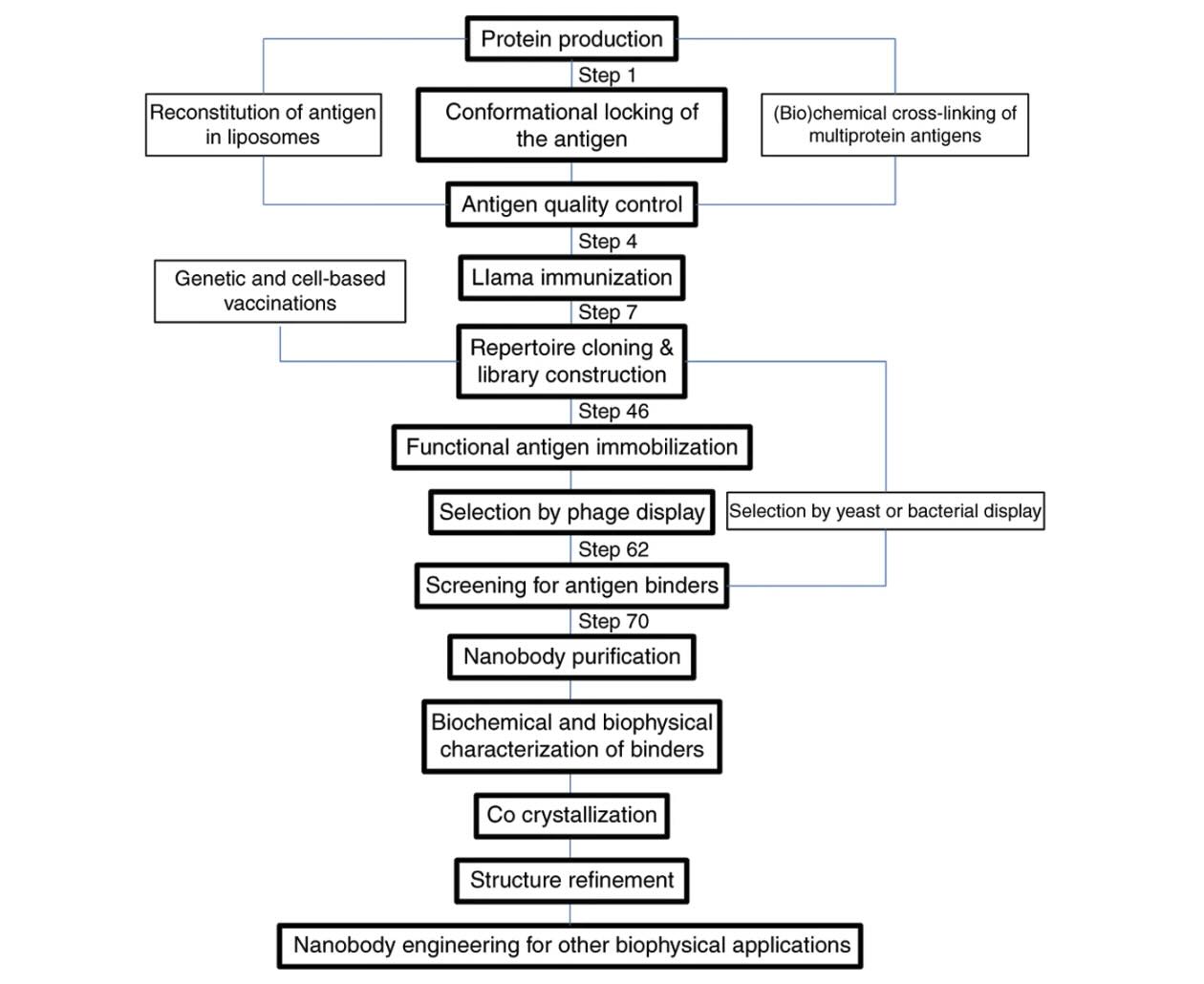
Explore how VHH antibodies stabilize protein conformations for crystallography, ……
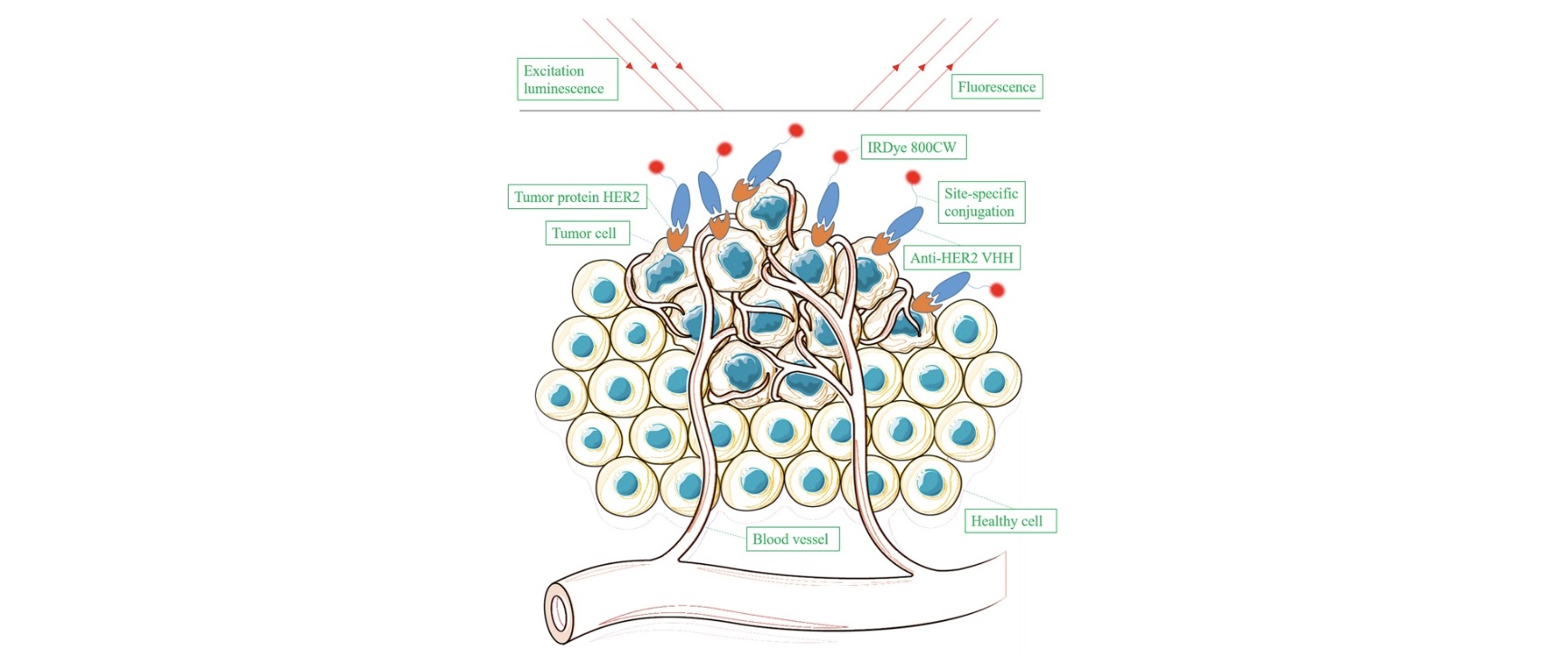
Explore VHH antibody production strategies for molecular imaging probes, includi……
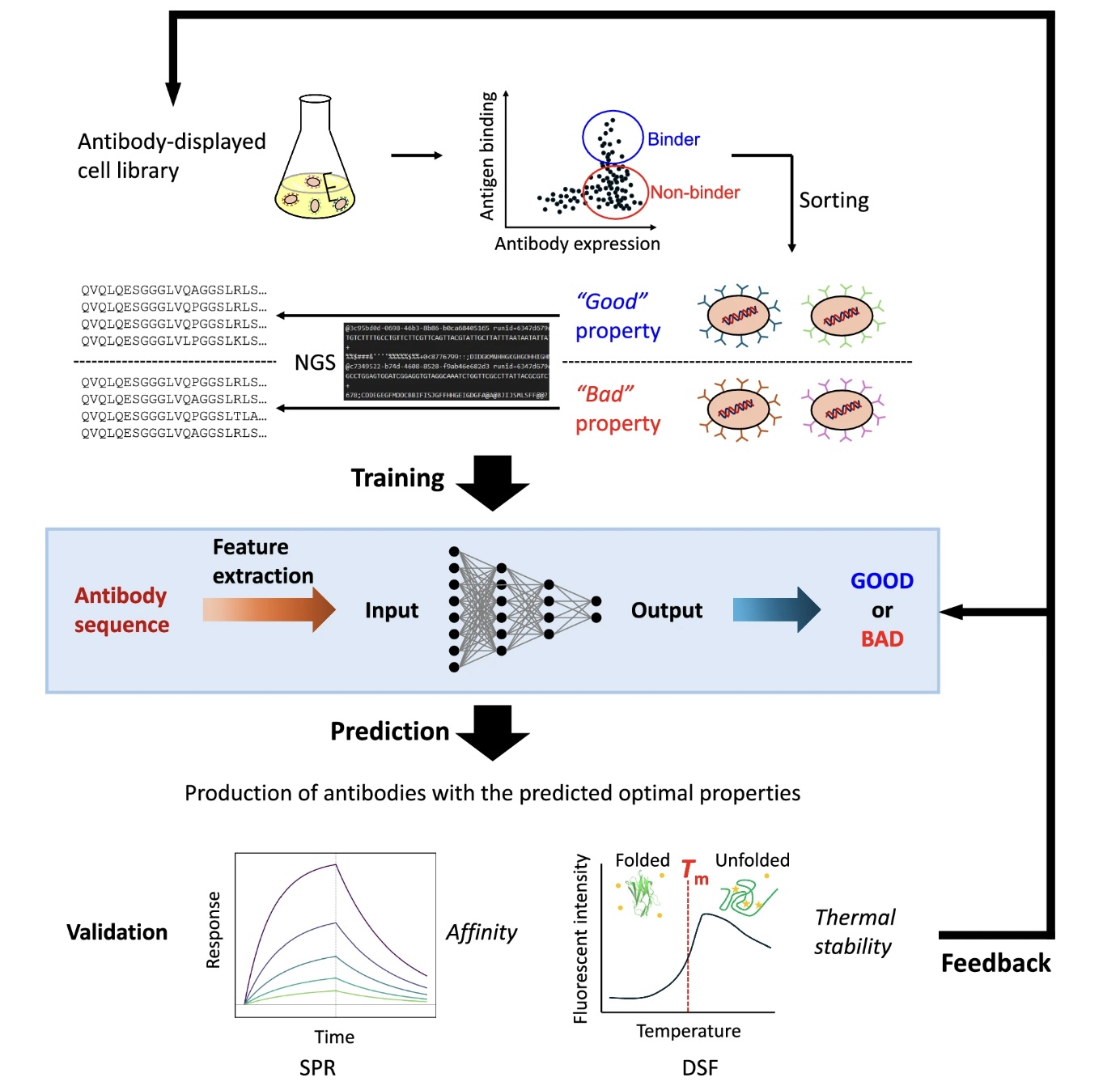
Artificial intelligence and machine learning are expanding the number of antibod……