Cancer remains a leading cause of death globally. Chemotherapies, while effective at killing rapidly dividing cells, lack specificity and often damage healthy tissue. This results in dose-limiting toxicities and restricts their applicability across cancer types. There is a clear need for therapies that offer both efficacy and selectivity.
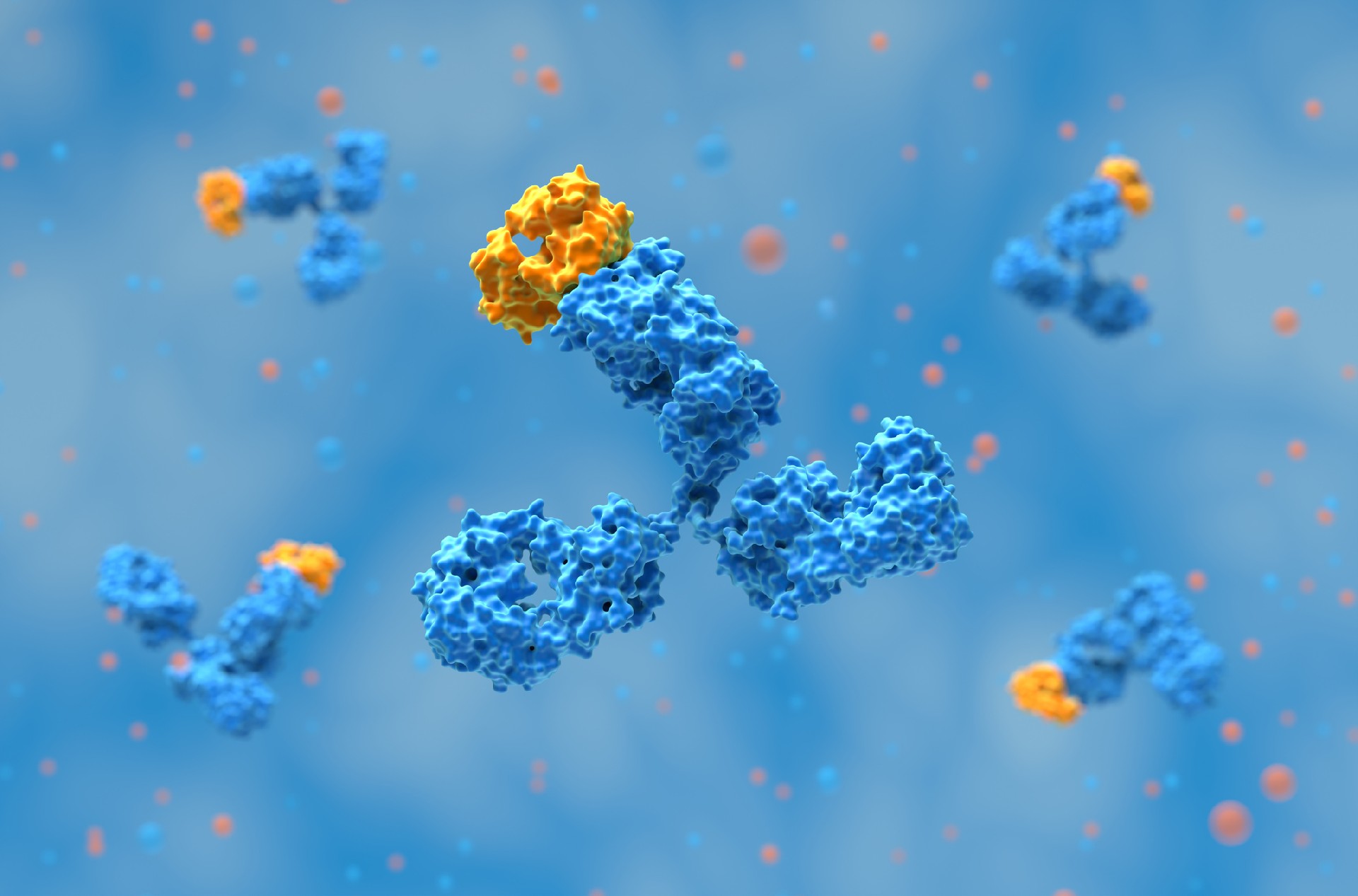
Antibody-drug conjugates (ADCs) address this need by using monoclonal antibodies to deliver cytotoxic agents directly to tumor cells. By targeting tumor-associated antigens, ADCs concentrate drug activity within cancerous tissue and reduce systemic exposure. This targeted delivery improves the therapeutic index and minimizes off-target effects.
Decades of development have led to clinically approved ADCs with demonstrated efficacy in hematologic and solid tumors. Early challenges, such as resistance and off-target toxicity, have been addressed through advances in antibody engineering and drug design, positioning ADCs as a validated and expanding modality in oncology.
Each ADC consists of:
A monoclonal antibody targeting a tumor-associated antigen
A cytotoxic payload
A chemical linker that connects the payload to the antibody
The integration of these components determines the specificity, potency, and safety of the final therapeutic product.
The monoclonal antibody serves as the targeting moiety, recognizing and binding to a tumor-associated antigen expressed on the surface of cancer cells. This targeting is critical for ensuring that the ADC selectively accumulates at the tumor site while minimizing interaction with normal tissues. The antigen selected must be highly expressed on malignant cells and exhibit minimal expression in healthy tissues to reduce the risk of on-target/off-tumor toxicity.
The payload is a highly potent cytotoxic agent that is intended to kill the target cell upon internalization and release. These agents are typically far more potent than conventional chemotherapeutics due to the limited number of molecules delivered per antibody. The payload must be chemically compatible with the linker and stable during systemic circulation to avoid premature release.
The linker is the covalent bridge between the antibody and the payload. While its specific chemical properties vary by design (e.g., cleavable vs. non-cleavable), its primary role at the structural level is to ensure that the ADC remains intact in circulation until it reaches the target cell. A well-designed linker also facilitates efficient release of the active drug once the ADC is internalized by the tumor cell. The overall architecture of the ADC must maintain stability, solubility, and homogeneity to meet regulatory and therapeutic standards.
Conventional conjugation methods used in early ADCs, such as random conjugation to lysine or reduced interchain cysteine residues, result in heterogeneous mixtures with variable drug-to-antibody ratios (DARs). This heterogeneity can impact pharmacokinetics, efficacy, and safety, as ADCs with high DARs may exhibit increased toxicity and faster clearance, while those with low DARs may be insufficiently potent.
To address this, site-specific conjugation strategies have been developed to control the exact location and number of payloads attached to each antibody molecule. These methods include the use of engineered cysteine residues, incorporation of unnatural amino acids, and enzymatic approaches such as microbial transglutaminase or glycan remodeling. Each approach allows for uniform DARs and improved batch-to-batch consistency, which is critical for therapeutic reproducibility and regulatory compliance.
Site-specific conjugation also enables better control over the physicochemical properties of the ADC, including solubility, aggregation tendency, and immunogenicity risk. By producing a more homogeneous product, manufacturers can achieve improved therapeutic windows and more predictable clinical outcomes. These techniques are now increasingly used in clinical-stage and commercial ADCs to meet the stringent quality and performance requirements of modern biologics.

The linker in an antibody-drug conjugate is responsible for maintaining the stability of the drug-antibody connection during circulation and enabling efficient payload release once the ADC is internalized. Linker chemistry directly influences the pharmacokinetics, safety profile, and therapeutic efficacy of the ADC, making it a critical element of design.
Linkers are broadly categorized into two types: cleavable and non-cleavable. Cleavable linkers are designed to release the cytotoxic payload in response to specific intracellular conditions such as acidic pH (acid-labile linkers), presence of certain enzymes (e.g., cathepsin B-sensitive peptide linkers), or reducing environments (disulfide linkers). These mechanisms allow for rapid and targeted release of the payload within the lysosome or cytoplasm of the cancer cell. However, cleavable linkers can be susceptible to premature cleavage in circulation, leading to off-target toxicity.
Non-cleavable linkers, by contrast, require complete degradation of the antibody in the lysosome before the payload is released. This often results in slower drug release but generally provides superior plasma stability and lower systemic toxicity. The choice between cleavable and non-cleavable linkers depends on the biological characteristics of the target tumor, the payload mechanism of action, and the desired pharmacokinetic profile. In either case, the linker must be stable enough to prevent premature drug release but labile enough to ensure efficient payload liberation at the target site.
Related: ADCs for In Vivo Research
Due to the limited number of antibodies that can bind each cancer cell, ADC payloads must be extremely cytotoxic, often with IC₅₀ values in the low nanomolar or picomolar range. Common payload classes include:
Microtubule inhibitors (e.g., auristatins, maytansinoids)
DNA-damaging agents (e.g., calicheamicin, duocarmycins)
Topoisomerase inhibitors (e.g., SN-38 derivatives)
In addition to potency, payloads must be chemically compatible with the linker and retain stability during bioconjugation, storage, and systemic circulation. The drug must remain inactive while attached to the antibody to prevent unintended cytotoxicity. Once released, it must act rapidly and irreversibly on the target cell to ensure efficacy. The structural and functional design of these small molecules is thus tightly integrated into the overall ADC development strategy.
The selection of a suitable target antigen is one of the most critical and challenging aspects of ADC development. An ideal target antigen is one that is highly and uniformly expressed on tumor cells, has minimal or no expression on normal tissues, and is accessible to circulating antibodies. This ensures that the ADC selectively binds to malignant cells, minimizing the risk of on-target/off-tumor toxicity.
Equally important is the internalization behavior of the antigen. Once bound by the antibody, the antigen-ADC complex must be internalized efficiently through receptor-mediated endocytosis. This intracellular trafficking is necessary for payload release, especially for cleavable linkers that rely on the intracellular environment to trigger drug liberation. Antigens that are poorly internalized result in reduced cytotoxicity, even if they are abundantly expressed on the cell surface.
Common antigens targeted by clinical ADCs include HER2, CD30, CD33, Trop-2, and Nectin-4. However, the range of viable targets is limited by tumor heterogeneity, antigen shedding, and expression in normal tissues. As a result, antigen discovery remains a bottleneck in expanding ADC applicability across additional cancer types. Biomarker-driven strategies and multi-omics profiling are increasingly employed to identify new antigens with the required specificity and internalization characteristics.

The therapeutic activity of an ADC depends not only on its ability to bind a target antigen but also on effective internalization and intracellular trafficking. Once the ADC binds to its specific cell surface antigen, the complex must be internalized via endocytosis and transported through the endosomal-lysosomal pathway. This intracellular routing is necessary to initiate payload release.
In the lysosome, ADCs with cleavable linkers rely on enzymatic degradation, acidic pH, or reducing conditions to trigger the release of the active drug. Non-cleavable linkers, by contrast, require complete proteolytic degradation of the antibody within the lysosome before the cytotoxic payload is liberated. The efficiency of this intracellular processing can significantly impact the cytotoxic potential of the ADC.
Poor internalization or impaired lysosomal trafficking can result in reduced payload release, leading to subtherapeutic drug concentrations at the target site. Furthermore, variability in internalization rates across different tumor types or even between patients may contribute to inconsistent clinical responses. As a result, early evaluation of internalization efficiency is a standard part of ADC target validation and development.
Clinical translation of ADCs is complex, involving the optimization of:
Antibody affinity and specificity
Linker stability and cleavage mechanism
Payload potency and mechanism of action
Drug-to-antibody ratio (DAR)
Tumor penetration and biodistribution
Each parameter impacts the ADC's pharmacokinetics, toxicity profile, and therapeutic index. Preclinical modeling and biomarker-driven patient selection are increasingly employed to guide clinical development and maximize clinical benefit.
Related: ADC Payloads: Expanding Beyond Microtubules and DNA-Damaging Agents
Manufacturing antibody-drug conjugates involves a complex, multi-stage bioprocess that integrates biologics production with small molecule synthesis and chemical conjugation. Each stage must be optimized to ensure consistency, product quality, and regulatory compliance. Unlike traditional biologics, ADCs require strict control over both biological and chemical parameters, making their manufacturing inherently more challenging.
Upstream processing begins with the production of the monoclonal antibody, typically in CHO (Chinese Hamster Ovary) cell lines, under conditions that ensure high yield and purity. Following purification, the antibody undergoes conjugation with the cytotoxic payload using defined chemical linkers. This step requires precise control over reaction conditions to achieve the desired drug-to-antibody ratio (DAR) while minimizing aggregation, free drug, or incomplete conjugation. Downstream purification processes are then used to remove unbound payloads and ensure product homogeneity.
Analytical characterization is critical at every stage, including assessment of DAR distribution, aggregation, stability, free drug levels, and potential immunogenicity. Regulatory agencies require thorough documentation of each parameter across development and commercial batches. Advances in site-specific conjugation techniques, high-resolution analytical tools, and scalable purification technologies have significantly improved the reproducibility and commercial feasibility of ADC manufacturing. As a result, contract development and manufacturing organizations (CDMOs) with integrated capabilities across biologics and chemistry are increasingly central to ADC supply chains.
As of 2025, over 15 ADCs have been approved by the FDA, with more than 100 candidates in clinical development. Notable approvals include trastuzumab emtansine (Kadcyla), brentuximab vedotin (Adcetris), and enfortumab vedotin (Padcev). The pipeline is diversifying beyond oncology, with early-stage programs exploring ADCs for autoimmune and infectious diseases. Innovations in bispecific ADCs, dual payloads, and novel cytotoxins continue to drive next-generation ADC development.
Future-generation ADCs are advancing through modifications to the antibody, linker, and payload components—each of which significantly influences pharmacological behavior. Even antibodies targeting the same antigen can vary in internalization efficiency and downstream trafficking. Notably, targeting mutant proteins such as oncogenic EGFR variants may enhance internalization due to elevated ubiquitination, potentially improving payload delivery and tumor specificity.
Bispecific ADCs represent another innovation, using engineered antibodies that bind two epitopes to promote receptor clustering and rapid internalization. Preclinical studies, including bispecific ADCs targeting HER2 and LAMP-3, have shown improved lysosomal delivery. Dual-payload ADCs are also in development, designed to deliver two cytotoxins with distinct mechanisms. A homogeneous anti-HER2 ADC with MMAE and MMAF demonstrated greater antitumor activity than single-payload variants in xenograft models, reducing resistance and enhancing efficacy.
Alternative ADC formats, including those based on polypeptides or single-chain fragments, are being explored to improve tumor penetration. PEN-221, for example, is a 2 kDa peptide-DM1 conjugate targeting somatostatin receptor 2. While smaller formats may clear rapidly from circulation, they offer potential for hard-to-access tumors. Non-internalizing ADCs are also under investigation, releasing payloads extracellularly in the tumor microenvironment for diffusion-based cell killing. Finally, novel payload classes—such as BCL-XL inhibitors in mirzotamab clezutoclax—are expanding the functional capabilities of ADCs beyond traditional cytotoxins.
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including HTP Recombinant Antibody Production, Bispecific Antibody Production, Large Scale Antibody Production, and Afucosylated Antibody Expression. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
References:
Fu, Z., Li, S., Han, S., Shi, C., & Zhang, Y. (2022). Antibody drug conjugate: The “biological missile” for targeted cancer therapy. Signal Transduction and Targeted Therapy, 7(1), 1-25. https://doi.org/10.1038/s41392-022-00947-7
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……