Immune Checkpoints
Immune checkpoints are regulatory pathways in the immune system that modulate immune responses and maintain self-tolerance. They are crucial for preventing autoimmune reactions but can be exploited by tumors to avoid immune destruction. These checkpoints act as "brakes" on the immune system, limiting the intensity and duration of immune responses to minimize damage to normal tissues.
Key Checkpoints: CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4); PD-1 (Programmed Death-1)
Mechanism of CTLA-4 Pathway
Expression: Primarily on activated T cells and regulatory T cells (Tregs).
Mechanism: Competes with CD28 for binding to B7 molecules (CD80/CD86) on antigen-presenting cells (APCs). B7-CD28 interaction provides a co-stimulatory signal necessary for full T-cell activation. CTLA-4 engagement delivers an inhibitory signal, dampening T-cell activation and proliferation.
Function: Modulates the intensity of the initial T-cell response in lymphoid organs, preventing overactivation.
Mechanism of PD-1 Pathway
Expression: On T cells, B cells, and some myeloid cells.
Mechanism: PD-1 interacts with its ligands PD-L1 (Programmed Death-Ligand 1) and PD-L2 on tumor cells and APCs. Ligand binding delivers an inhibitory signal to the T cell, reducing its activity and promoting T-cell exhaustion. This checkpoint functions at the effector phase in peripheral tissues and the tumor microenvironment.
Function: Limits T-cell activity to prevent tissue damage during inflammation and to maintain tolerance in the tumor microenvironment.
Rationale for Immune Checkpoint Inhibition
Tumor Immune Evasion
Mechanisms: Tumors often overexpress PD-L1, exploiting PD-1 on T cells to suppress immune responses. Tumors attract regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs) that express checkpoint molecules like CTLA-4. The tumor microenvironment is enriched with factors that promote immune tolerance and inhibit effector T-cell function.
Therapeutic Strategy
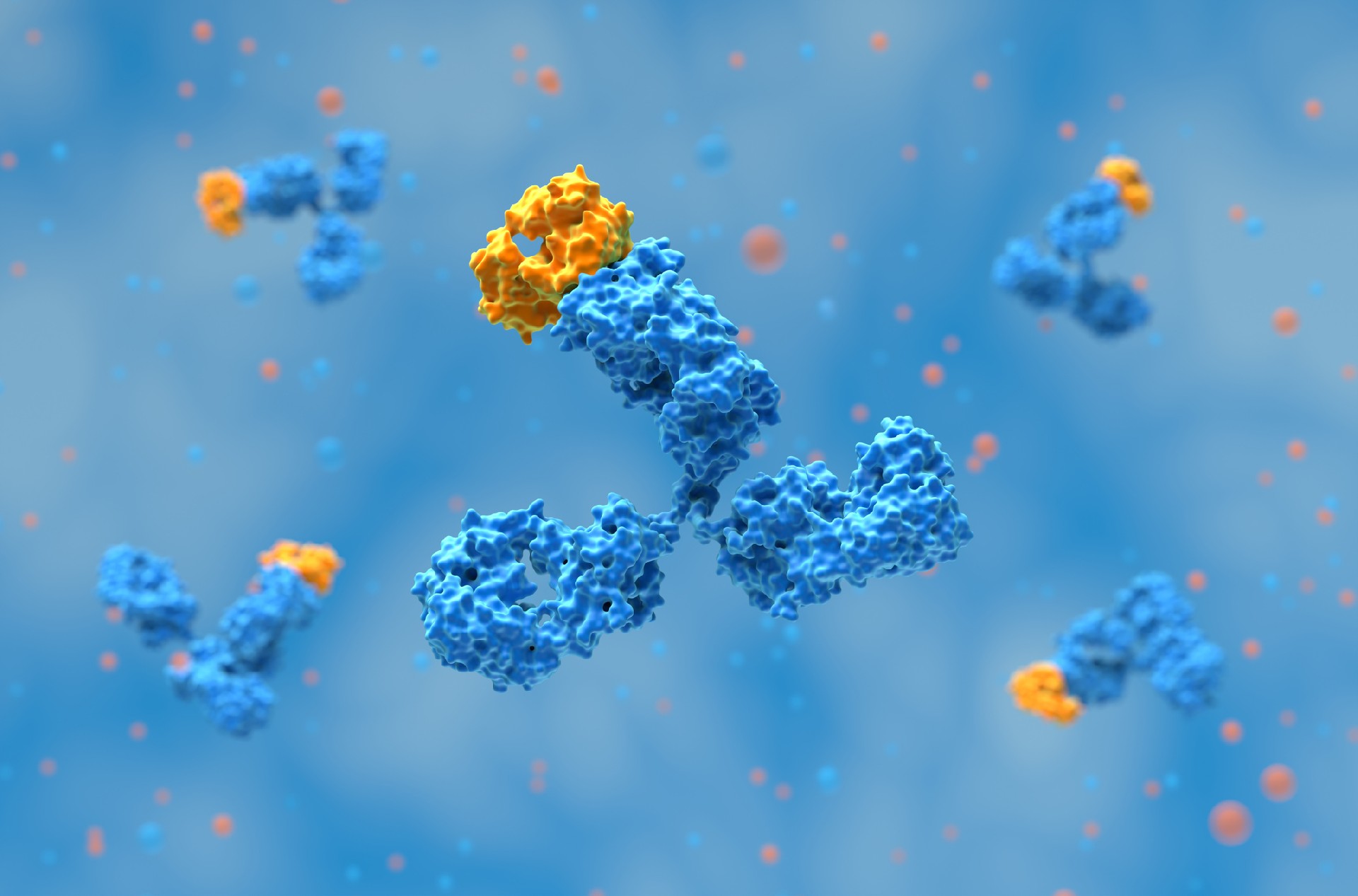
Checkpoint Blockade: Monoclonal antibodies targeting CTLA-4 or PD-1/PD-L1 can disrupt inhibitory signals and restore T-cell activation. Indications: Effective particularly in cancers with:
High Mutational Burden: Generates neoantigens that can be recognized by T cells.
Inflamed Tumor Microenvironment: Presence of T cells and high expression of checkpoint ligands make them more susceptible to checkpoint blockade.
Clinical Significance
Restoring T-cell Function: Blockade of CTLA-4 and PD-1/PD-L1 pathways can reinvigorate exhausted T cells, enhancing their ability to attack tumor cells.
Tumor-Specific Response: Checkpoint inhibitors can potentially re-establish a targeted immune response against tumor antigens, leading to tumor regression.
Durable Responses: Clinical trials have shown that checkpoint inhibition can lead to long-lasting remissions in certain cancers, suggesting a sustained immune memory response.
Therapeutics
Anti-CTLA-4 Therapy: Ipilimumab is an mAbapproved to treat advanced melanoma, renal cell carcinoma, and others. It works by binding to CTLA-4, preventing its inhibitory signal, thereby enhancing T-cell priming and proliferation. Ipilimumab was the first checkpoint inhibitor approved for melanoma, and ongoing research is exploring its efficacy with other therapies in a variety of cancers.
Anti-PD-1/PD-L1 Therapy: Pembrolizumab is an anti-PD-1 humanized antibody approved to treat advanced melanoma, non-small cell lung cancer (NSCLC), head and neck cancer, and others. It demonstrated significant improvements in overall survival and progression-free survival in various cancers.
Combination Therapies: Combining immune checkpoint inhibitors with other treatments, such as chemotherapy, targeted therapy, or additional checkpoint inhibitors, can enhance anti-tumor efficacy by attacking cancer through multiple mechanisms. Dual checkpoint inhibition, exemplified by nivolumab (anti-PD-1) and ipilimumab (anti-CTLA-4), improves both T-cell priming and effector functions, leading to better survival outcomes in cancers like melanoma and renal cell carcinoma. Chemoimmunotherapy leverages chemotherapy-induced immunogenic cell death to boost checkpoint inhibitor effectiveness, as seen with pembrolizumab in non-small cell lung cancer (NSCLC). Combining checkpoint inhibitors with targeted therapies, like atezolizumab and VEGF inhibitors in renal cell carcinoma, modulates the tumor microenvironment and enhances immune responses. While combination therapies can achieve significant clinical benefits, they often come with increased immune-related adverse events, necessitating careful patient selection and optimization of dosing regimens.
Emerging Checkpoint Targets

Two popular topics discussed at the 2026 BIO International Convention were devel……
AI is changing antibody discovery, but model performance depends on the quality ……
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……