Welcome to Antibody Basics by Biointron, Part 8. In this episode, we’ll talk about therapeutics targeting cancer.
Cancer immunotherapy leverages the body's immune system to fight cancer more selectively and effectively than traditional methods such as chemotherapy and radiation. Types: Monoclonal antibodies, checkpoint inhibitors, cancer vaccines, CAR T-cell therapy, and oncolytic virus therapy.
The road towards cancer immunotherapy:
1890s: Early observations: William Coley, a surgeon, observed spontaneous remission in cancer patients after a bacterial infection. This sparked the concept of harnessing the immune system to fight cancer.
1940s - 1970s: Interest in the immune system: Discoveries of interferons, T cells, dendritic cells, and natural killer cell (NK cells) activity.
1980s: Monoclonal antibodies and CAR T-cell therapy: The development of techniques for creating targeted antibodies and engineering immune cells opened doors for novel immunotherapy approaches.
1990s - 2000s: Checkpoint inhibitors: The identification of molecules like CTLA-4 and PD-1 that suppress immune responses led to the development of checkpoint inhibitor drugs.
2010s - Present: Era of new therapies: Current research focuses on tailoring immunotherapy to specific cancers, new modalities, and the combination of technologies such as AI.
Targeted Delivery: Targeted delivery in cancer therapy involves the design of drugs or therapeutic agents that are directed specifically to the tumor site, minimizing exposure to healthy tissues. This precision not only enhances the therapeutic efficacy but also reduces the side effects typically associated with conventional chemotherapy. E.g. Antibody-drug conjugates (ADCs), where antibodies direct cytotoxic drugs to cancer cells, or through liposomal delivery systems that encapsulate drugs and release them in response to specific tumor microenvironment conditions.
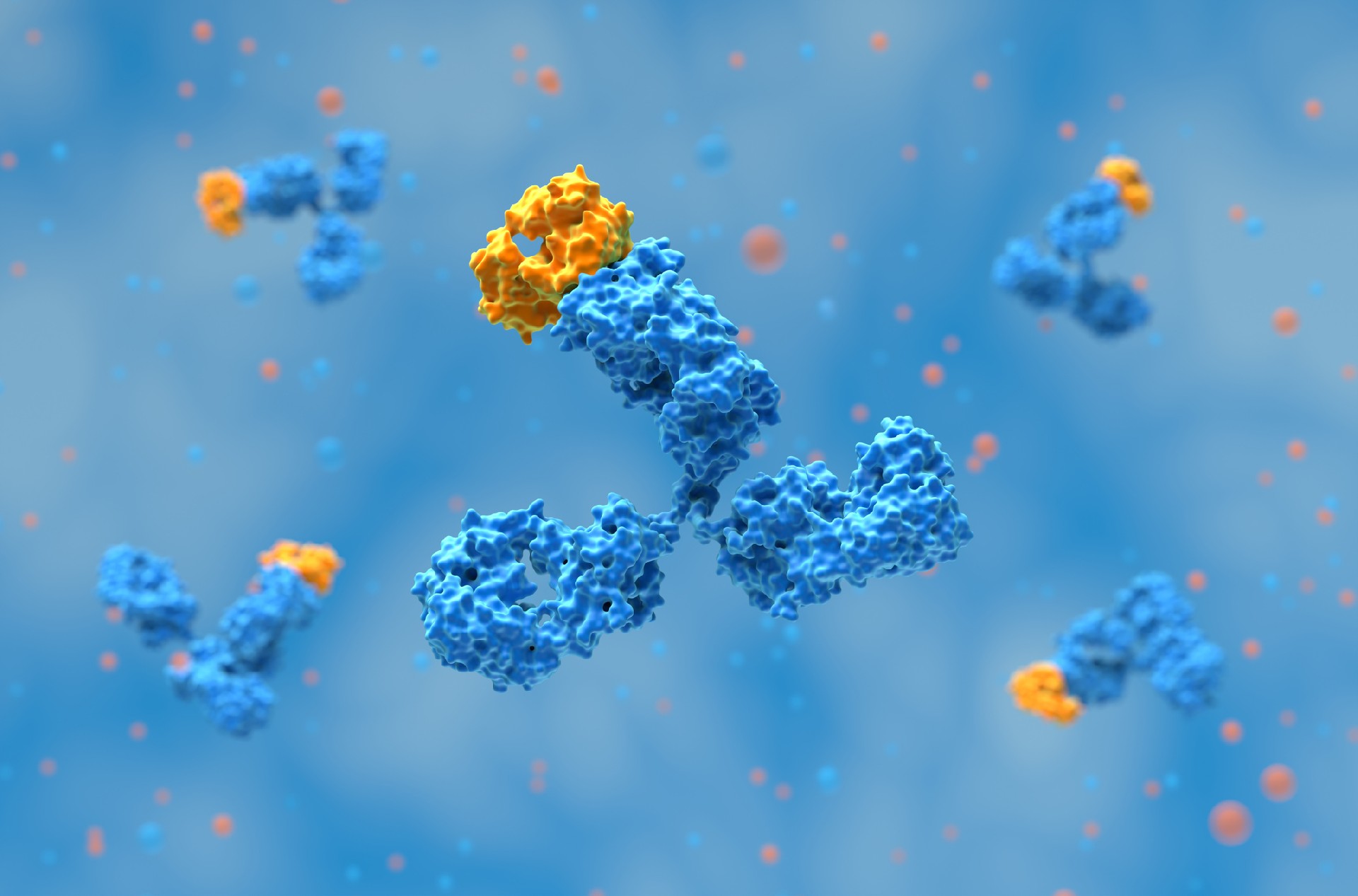
Tumor Selectivity: High tumor selectivity is critical to maximizing therapeutic success and minimizing harm to normal tissues. Selectivity can be achieved by exploiting the unique biological characteristics of tumor cells, such as overexpressed receptors or mutated proteins not found in healthy cells. One of the most successful examples of tumor selectivity is the use of monoclonal antibodies that target specific antigens or receptors overexpressed on the surfaces of tumor cells, such as HER2 in breast cancer. Services like Biointron’s CHOK1BN cell line commercial license provide a foundation for such targeted therapies.
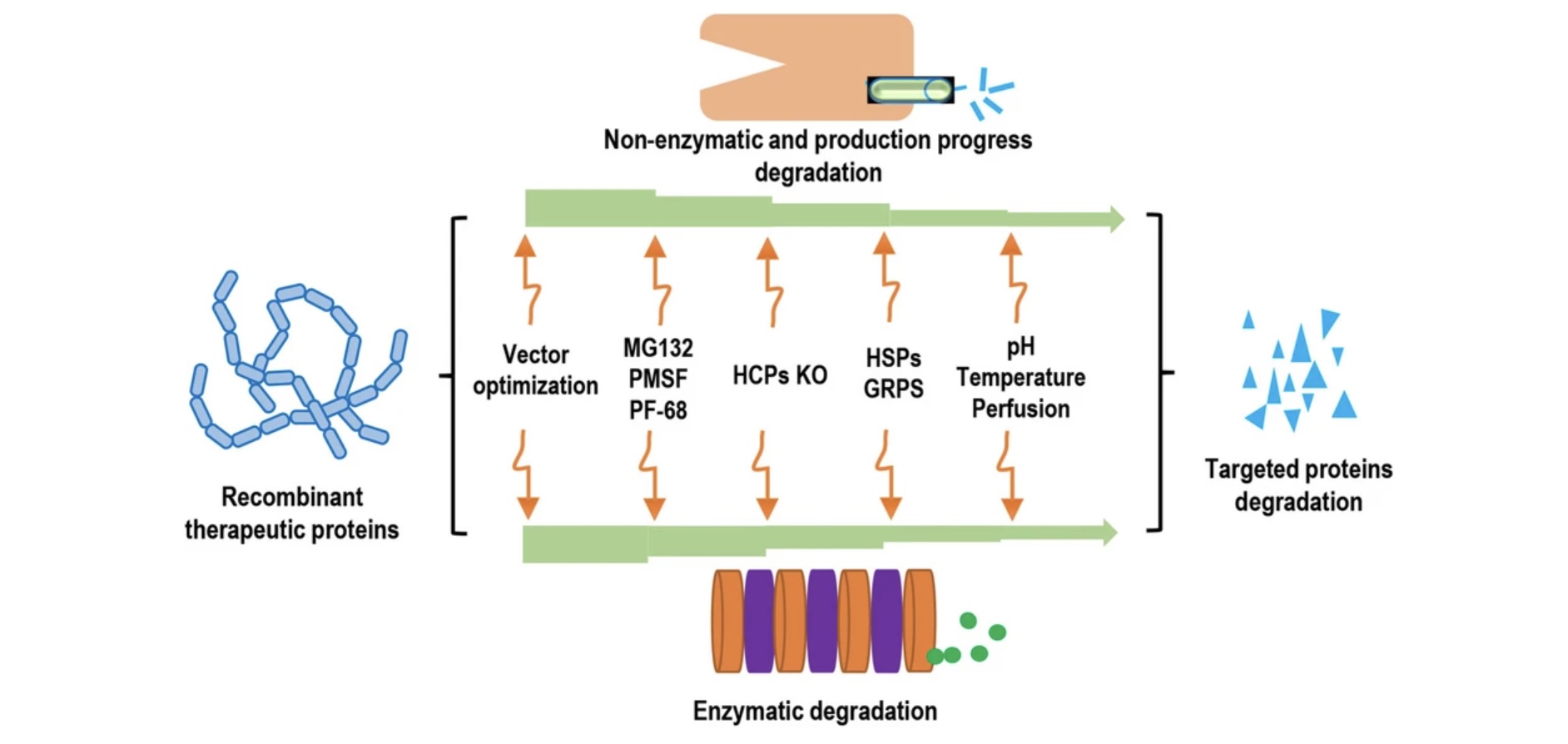
Stability: A drug must remain stable long enough to reach its target without degradation or premature release of its active components. Major challenges include the degradation of drugs by enzymes and immune clearance, so researchers may modify molecular structures, add protective coatings, or use delivery vehicles for the drugs.
Rituximab (Rituxan): Approved in 1997, it targets CD20 to treat non-Hodgkin lymphoma. It is one of the first monoclonal antibodies to be approved for cancer.
Trastuzumab (Herceptin): Approved in 1998, it targets HER2 to treat breast cancer. By attaching to the growth factor antigen, it stops the breast cancer cells from growing and dividing.
Ipilimumab (Yervoy): Approved in 2011, it targets CTLA-4 to treat metastatic melanoma. It is the first checkpoint inhibitor approved by the FDA.
Nivolumab (Opdivo): Approved in 2014, it targets PD-1 to treat melanoma and non-small cell lung cancer. It is also a checkpoint inhibitor.
Resistance issues: Acquired therapeutic resistance against antibodies is a major challenge. This can happen due to: a mutation present in the tumor before start of the treatment; continuous immune selection pressure of the treatment causing subsequent changes in signaling of survival pathways; epithelial-to-mesenchymal transition (EMT) resulting in loss of cell-to-cell contact and becoming more migratory, promoting stem cells characteristics; lower or heterogeneous expression of antigens and inhibition of complement dependent cytotoxicity.
MHC class I expression: Each cancer cell differs from healthy cells around the tumor by >11,000 genomic mutations. While some may lead to tumor-associated antigens expressed on the cell's surface to become drug targets, others may lose their MHC class I expression. The major histocompatibility complex is a group of genes that code for proteins on cell surfaces, helping the immune system recognize foreign substances. They’re necessary for distinguishing between self and non-self cells and for presenting antigens to T cells. Thus, losing MHC class I expression hampers the effectiveness of immunotherapies that rely on the recognition of MHC-presented antigens by the immune system.
ADCs: Antibody-drug conjugates are an emerging modality that combine a monoclonal antibody with a cytotoxic payload, allowing them to deliver therapy more efficiently than conventional chemotherapy. Kadcyla (trastuzumab emtansine) is an ADC that improves upon the success of Herceptin by linking it to a potent cytotoxic drug, DM1. Besides, ADCs, antibody- small interfering RNA (siRNA) conjugates and antibody-cytokine fusions are drawing more interest.
Multispecifics: Multispecific antibodies like bispecifics and trispecifics are useful for cancer, as more than one mediator contributes to the activation of cancer-related signaling pathways. In cancer immunotherapy, several mechanisms have been developed: engaging T cells or other immune cells (e.g., NK cells) to specifically eliminate tumor cells; bridging receptors to block or activate synergistic signaling pathways; targeting multiple tumor antigens or different antigen epitopes on tumor cells to increase tumor selectivity.
Personalized cancer treatments: The potential future of personalized medicine for cancer may be with therapeutic antibodies. Delgado & Garcia-Sanz (2023) proposes screening a large panel of antibodies with each patient’s tumor sample to design initial treatment combinations containing two–three antibodies. This would allow killing of the maximum number of tumor cells, in addition to having a backup or additional combinations of antibodies with chemotherapeutics or inhibitors.
For tailored solutions in antibody development, explore Biointron's CHO-K1 stable cell line generation service for advanced techniques and optimized cell line engineering.
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……