Antibody-Drug Conjugates (ADCs) are a breakthrough in oncology, integrating the targeting precision of monoclonal antibodies (mAbs) with the potent cytotoxic effects of traditional chemotherapy. Their design aims to improve cancer treatment by ensuring that powerful anti-cancer drugs reach and destroy tumor cells while minimizing damage to healthy tissues. This article provides a detailed exploration of ADCs, from their structural components to their clinical applications and the innovative approaches in their manufacturing.
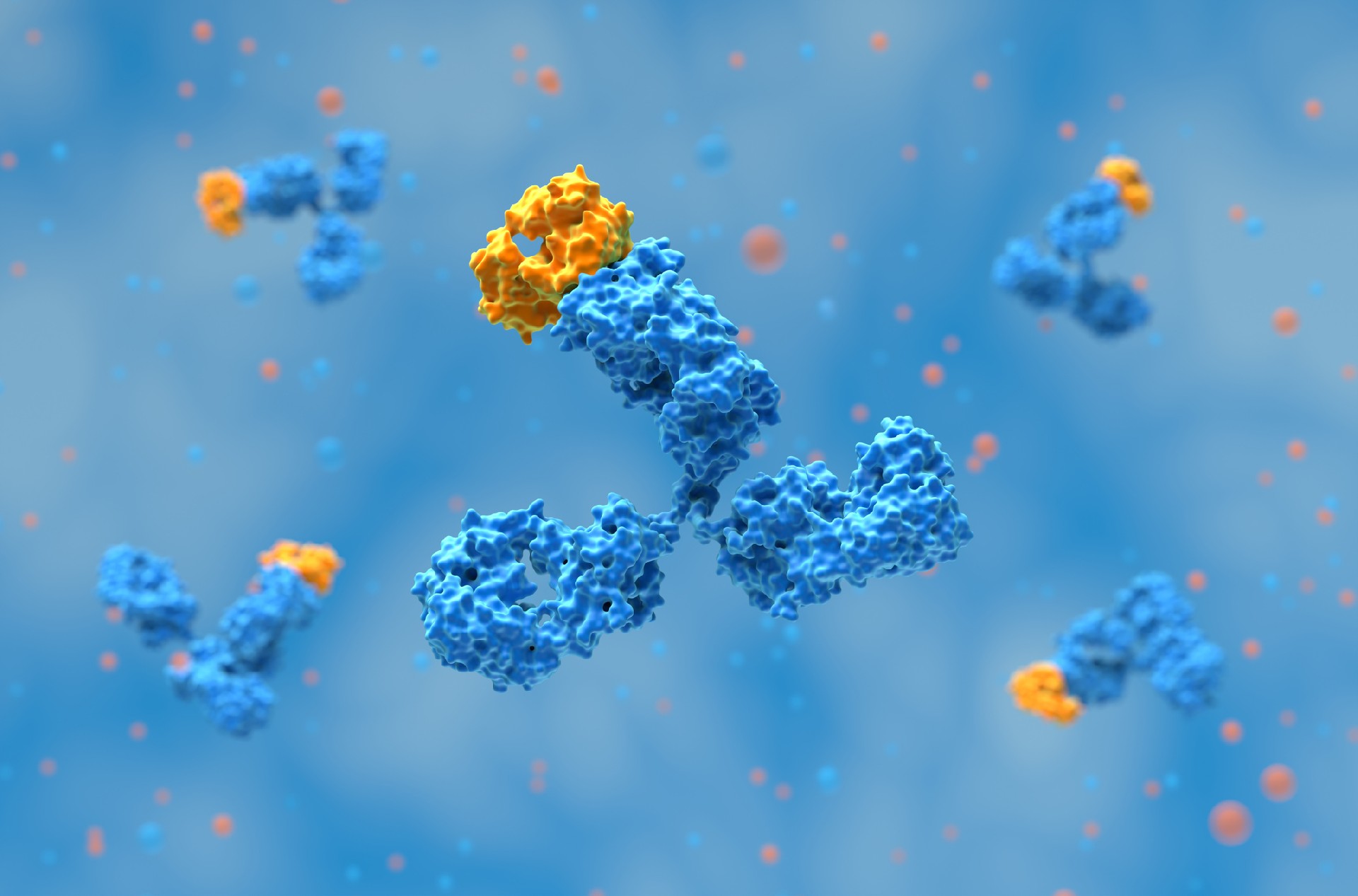
ADCs are complex molecules consisting of three main components: a monoclonal antibody, a chemical linker, and a cytotoxic payload. Each component plays a critical role in the efficacy and specificity of ADCs. Monoclonal antibodies (mAbs) form the backbone of ADCs, guiding the toxic payload to cancer cells. These antibodies are engineered to recognize and bind specifically to antigens present on tumor cells. The most common type used in ADCs is the IgG1 isotype due to its favorable properties, including a long serum half-life and strong immune effector functions like antibody-dependent cellular cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC).
To address limitations such as the large size and poor tumor penetration of full-size antibodies, researchers are developing antibody fragments like single-chain variable fragments (scFvs) and diabodies. These smaller formats retain the targeting capability of full-size antibodies but offer better tumor penetration and reduced systemic accumulation, potentially leading to more effective treatments for solid tumors.
Linkers are chemical moieties that attach the cytotoxic drug to the antibody. They are designed to be stable in the bloodstream but to release the payload upon reaching the target cell. Linkers can be cleavable or non-cleavable. Cleavable linkers, such as those responsive to the acidic environment of lysosomes or the presence of specific enzymes, are widely used due to their ability to release the drug selectively within tumor cells. Non-cleavable linkers, on the other hand, ensure that the drug remains attached to the antibody until the entire ADC is degraded within the cell, thereby minimizing off-target effects.
The payloads used in ADCs are highly potent cytotoxic agents. They must be powerful enough to kill cancer cells at very low concentrations since only a small fraction of the administered ADC reaches the tumor. Common payloads include DNA-damaging agents like calicheamicin and tubulin inhibitors like auristatins and maytansinoids. These drugs interfere with vital cellular processes such as DNA replication and microtubule formation, leading to cell death.
Targeting and Binding: The antibody component of the ADC binds to a specific antigen on the surface of cancer cells.
Internalization: The ADC-antigen complex is internalized by the cancer cell through endocytosis.
Drug Release: Once inside the cell, the linker is cleaved (if cleavable), or the entire ADC is degraded, releasing the cytotoxic drug.
Cytotoxicity: The released drug exerts its cytotoxic effect, leading to cell death.
This targeted delivery system enhances the therapeutic index of the drug, increasing its efficacy against cancer cells while reducing systemic toxicity.
To date, numerous ADCs have been approved by regulatory agencies such as the FDA and EMA for the treatment of various cancers. Some of the notable ones include:
Gemtuzumab Ozogamicin (Mylotarg®): Approved for acute myeloid leukemia (AML), it targets the CD33 antigen on leukemia cells and delivers the DNA-damaging agent calicheamicin.
Brentuximab Vedotin (Adcetris®): Targets CD30 in Hodgkin lymphoma and anaplastic large cell lymphoma, delivering the tubulin inhibitor MMAE.
Trastuzumab Emtansine (Kadcyla®): Used for HER2-positive breast cancer, it combines trastuzumab's targeting of HER2 with the microtubule inhibitor DM1.
Sacituzumab Govitecan (Trodelvy®): Approved for triple-negative breast cancer, it targets TROP-2 and delivers the topoisomerase inhibitor SN-38.
Despite the success of ADCs, several challenges remain. The development process is complex and expensive, requiring precise control over the conjugation chemistry to ensure product consistency and efficacy. Additionally, ADCs can still cause side effects, often related to the cytotoxic payloads. For instance, hematological toxicities, peripheral neuropathy, and liver toxicity are common.
Researchers are exploring several strategies to overcome these challenges:
Improved Conjugation Methods: Site-specific conjugation techniques can produce more homogeneous ADC preparations with a controlled drug-to-antibody ratio (DAR), enhancing therapeutic efficacy and reducing side effects.
Novel Payloads and Linkers: Developing new cytotoxic agents and more stable linkers can enhance the specificity and potency of ADCs.
Combination Therapies: Combining ADCs with other treatments, such as immune checkpoint inhibitors or traditional chemotherapies, may enhance their efficacy and overcome resistance mechanisms.
ADCs represent a significant advancement in targeted cancer therapy, offering the potential to deliver powerful cytotoxic drugs directly to tumor cells while sparing healthy tissues. Continued research and development are likely to expand their applications beyond oncology, potentially transforming the treatment landscape for a variety of diseases.
References:
Riccardi, F., Dal Bo, M., Macor, P., & Toffoli, G. (2023). A comprehensive overview on antibody-drug conjugates: From the conceptualization to cancer therapy. Frontiers in Pharmacology, 14, 1274088. https://doi.org/10.3389/fphar.2023.1274088
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……