Bispecific antibodies (BsAbs) represent a major advancement in immunotherapy by enabling the simultaneous targeting of two different antigens. Blinatumomab (Blincyto, Amgen) was the first bispecific T-cell engager (BiTE) antibody approved for oncology, marking a significant breakthrough in the treatment of B-cell malignancies. This article reviews the development, mechanism of action, clinical efficacy, and impact of blinatumomab on the evolving landscape of targeted cancer therapies.
Traditional monoclonal antibodies targeting B-cell malignancies, such as rituximab (anti-CD20), improved treatment outcomes but did not fully eliminate residual disease in relapsed or refractory (R/R) patients. In B-cell acute lymphoblastic leukemia (B-ALL), minimal residual disease (MRD) remains a significant predictor of relapse and poor overall survival. Bispecific antibodies were designed to directly engage the patient’s immune system, specifically T cells, to eliminate residual cancer cells that evade conventional therapies.1
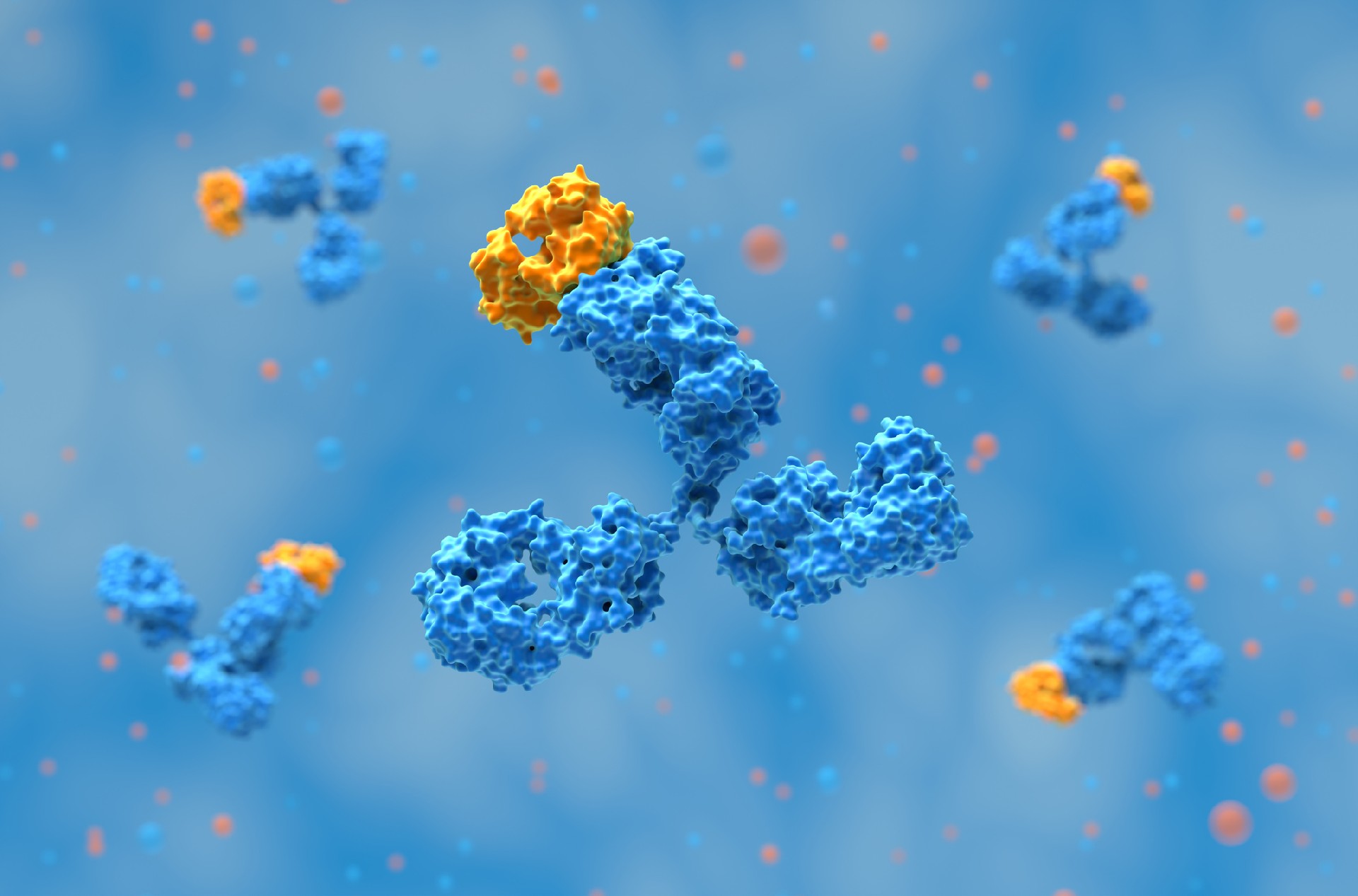
Blinatumomab is a bispecific T-cell engager (BiTE) antibody composed of two single-chain variable fragments (scFvs):
One scFv binds to CD19, a surface antigen universally expressed on B-cell malignancies.
The other scFv binds to CD3, a component of the T-cell receptor complex, activating T cells.
The small 55 kDa size of blinatumomab enhances tumor penetration compared to full-length monoclonal antibodies. Once bound, it brings T cells into direct proximity with CD19+ cancer cells, triggering T-cell activation and cytotoxicity. The activated T cells release perforin and granzymes, leading to apoptosis of target cells. Importantly, T-cell engagement is independent of major histocompatibility complex (MHC) presentation, allowing blinatumomab to bypass immune evasion mechanisms.

Bispecific T cell engagers (BiTEs) have emerged as a promising immunotherapy approach in the treatment of hematologic malignancies by leveraging the body's immune system to target tumor cells. Since Blinatumomab’s approval in 2014, extensive research has focused on optimizing BiTE therapy by refining molecular structures, improving treatment regimens, and addressing challenges such as immune evasion and resistance. Various bispecific T cell-recruiting antibodies have been developed based on the BiTE platform, expanding the therapeutic landscape for multiple hematologic cancers.
Structurally, bispecific antibodies (BsAbs) can be categorized based on their targets and molecular design. BiTEs, belonging to the class of BsAbs that engage both tumor antigens and immune-related molecules, are composed of two single-chain variable fragments (scFvs) connected by a linker, allowing simultaneous binding to CD3 on T cells and a tumor antigen. Advances in BsAb engineering, including IgG-based platforms such as DuoBody, CrossMab, and XmAb, have improved stability and half-life, while novel formats like DART and TandAb have enhanced binding affinity and cytotoxic activity. These innovations address some of the limitations of early BiTEs, including their short half-life and requirement for continuous infusion.
To further enhance BiTE efficacy, combination therapies with immune checkpoint inhibitors, such as PD-1/PD-L1 blockers, are being explored to overcome immune resistance. Additionally, emerging bispecific antibodies targeting CD123, CD33, and FLT3 in acute myeloid leukemia (AML), as well as BCMA and GPRC5D in multiple myeloma, highlight the expanding potential of BiTE therapy across hematologic malignancies.
Despite their promise, BiTEs face limitations, including antigen escape and the need for continuous administration. Strategies to counteract tumor resistance, such as dual-targeting bispecific antibodies and novel combination regimens, are currently under investigation. As research continues to refine BiTE technology, their role in the treatment paradigm of hematologic malignancies is expected to expand, offering targeted and effective treatment options for patients with otherwise limited therapeutic choices.2

In vitro studies demonstrated that blinatumomab was 100- to 10,000-fold more effective at tumor cell lysis than earlier bispecific constructs.
In vivo models, including xenograft studies in mice and non-human primates, confirmed significant tumor regression with low systemic toxicity.
Blinatumomab exhibited a short half-life (~2 hours), necessitating continuous intravenous infusion for sustained efficacy.
First-in-human trials (2001): 21 patients with relapsed/refractory B-NHL and one with chronic lymphocytic leukemia (CLL) received blinatumomab as intermittent IV infusions. The trial was halted due to neurological toxicities and lack of objective response.
Phase I Dose-Escalation (2004): A continuous IV infusion schedule (60 μg/m²/day) was established, improving drug exposure and response rates. However, neurological toxicities remained a dose-limiting factor.
Phase II B-NHL Studies: Blinatumomab achieved an overall response (OR) rate of 69%, with the highest responses in follicular lymphoma (80%) and mantle cell lymphoma (71%).
GMALL Phase II Trial (2008):
Enrolled adults in complete remission but with MRD persistence after chemotherapy.
80% of patients achieved MRD negativity after one cycle.
Long-term follow-up showed 50% remained in remission at 50 months.
BLAST Trial (2010–2018):
113 patients with MRD+ B-ALL.
78% achieved MRD negativity after one cycle.
Median relapse-free survival (RFS) of 18.9 months.
FDA approval in 2018 for MRD-positive B-ALL.
Phase II GMALL Study (2010):
Evaluated R/R B-ALL patients, leading to 69% CR/CRh rate.
Median overall survival (OS) 13.0 months.
Phase III TOWER Trial (2014–2017):
Compared blinatumomab vs. standard chemotherapy in R/R B-ALL.
Blinatumomab significantly improved OS (7.7 vs. 4.0 months, HR 0.71, p=0.01).
CR/CRh rates: 44% (blinatumomab) vs. 25% (chemotherapy).
Established blinatumomab as a standard of care in R/R B-ALL.
ALCANTARA Study (2014–2017) – Ph+ B-ALL:
Evaluated Philadelphia chromosome-positive (Ph+) R/R B-ALL patients.
36% achieved CR, with an MRD negativity rate of 88%.
Led to FDA approval for Ph+ B-ALL in 2017.
Phase I/II Pediatric Study (2016):
70 children with R/R B-ALL.
39% achieved CR, with MRD negativity in 14 patients.
34% proceeded to HSCT.

Cytokine Release Syndrome (CRS): Occurs due to rapid T-cell activation and cytokine release (IL-6, TNF-α). It is managed with stepwise dosing (9 → 28 μg/day) and dexamethasone premedication. The incidence is Grade 3 CRS ~2–5%.
Neurotoxicity: Common symptoms include tremor, confusion, seizures, and encephalopathy. It is observed in up to 50% of patients, but Grade ≥3 cases were 9–20%. The short half-life (~2 hours) allows rapid symptom resolution upon drug discontinuation.
Combination therapies: Blinatumomab + immune checkpoint inhibitors (Nivolumab, Ipilimumab).
Use in frontline ALL therapy: Ongoing trials incorporating blinatumomab with standard chemotherapy.
Alternate delivery methods: Subcutaneous administration to improve patient convenience.
Blinatumomab in Non-Hodgkin Lymphoma (NHL):
Phase II trials in relapsed/refractory diffuse large B-cell lymphoma (DLBCL).
Ongoing studies evaluating combination with lenalidomide.

Blinatumomab’s approval as the first bispecific antibody in oncology marked a major advancement in immunotherapy. Its efficacy in R/R B-ALL and MRD+ disease has reshaped treatment paradigms, offering a targeted approach for patients who previously had limited options. As bispecific antibody technology evolves, blinatumomab paves the way for next-generation therapies in hematologic and solid tumors.
Related: Pivotal Moments in Oncology Antibody Drug Development
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including Bispecific Antibody Production. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Blinatumomab, a bispecific B-cell and T-cell engaging antibody, in the treatment of B-cell malignancies. (2019). Human Vaccines & Immunotherapeutics. https://doi.org/10.1080/21645515.2018.1540828
Tian, Z., Liu, M., Zhang, Y., & Wang, X. (2021). Bispecific T cell engagers: an emerging therapy for management of hematologic malignancies. Journal of Hematology & Oncology, 14(1). https://doi.org/10.1186/s13045-021-01084-4
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……