In mammals, antibodies are classified into five major isotypes: IgA, IgD, IgE, IgG, and IgM. Each isotype is defined by the heavy chain it contains: alpha (IgA), delta (IgD), epsilon (IgE), gamma (IgG), or mu (IgM). These structural differences in the heavy chains determine the antibody's function, tissue localization, and role in the immune response. Furthermore, antibody light chains fall into two classes—kappa and lambda—with kappa being more common, though both exhibit similar functions despite differences in sequence.
Understanding the structural variations across antibody isotypes is crucial in therapeutic antibody development, where specific isotypes can be leveraged to elicit desired immune responses, enhance bioavailability, or improve stability in various clinical applications.

Immunoglobulins, also known as antibodies, are heterodimeric proteins made up of two heavy (H) chains and two light (L) chains. They can be classified into five primary isotypes (IgG, IgA, IgD, IgE, and IgM) determined by the constant domains in their H chains, which give each isotype their different characteristics.
Immunoglobulin G is the most abundant subtype, being present in the largest concentrations at 75-80% of IgGs in blood and tissue fluids. IgG makes direct impacts on the immune response with high neutralization and opsonization activities towards toxins and viruses, acting as the first line of defense after memory B cells trigger a response. They are responsible for both existing and acquired immunity against previously encountered antigens. Once IgG binds to antigens, the Fc receptor can bind to macrophages, which can carry out phagocytosis on the intruder.1,2
Uniquely, IgG can also cross the placenta and impart immunity to the fetus. This occurs through transcytosis, in which the IgG is endocytosed and shuttled across the cytoplasm to be secreted towards the basal cell membrane of syncytiotrophoblasts. Once there, the complex is released into fetal circulation.
IgG can be further classified into: IgG1, IgG2, IgG3, and IgG4. All four subtypes exhibit different functional activities. For example, with a HIV patient, IgG3 antibodies have been demonstrated to be more effective at neutralizing HIV over IgG1, likely because of differing antibody flexibility affecting access and how changes are induced in the virus’ oligomer structure.3

Immunoglobulin M is the first isotype to be expressed by the adaptive immune system in response to a foreign pathogen, during B cell development. It is typically present as the antigen receptor on the naïve B-cell surface, allow for the B cell to associate with the polypeptides CD79a and CD79b, which play roles in IgM cell signaling.
IgM is monomeric when first produced by plasma cells but when secreted can link to other IgM units to form a pentameric configuration containing a polypeptide J-chain. This occurs during maturation and antigenic stimulation and increases IgM’s avidity since there would be ten antigen-binding sites per pentameric molecule. Through interactions with the antigen, IgM can then opsonize it for destruction.
The detection of IgM can be used to diagnose patients from acute exposure to a pathogen, since IgM is typically linked with a primary immune response. However, it does not indicate whether the patient still has that pathogen or if it had been eliminated, since memory plasma cells help form immunological memory to generate antibodies against a pathogen for many more months and years to come.4
In addition, several disorders can be connected with IgM, such as X-linked Hyper-IgM Syndrome. This is a rare primary immune deficiency disorder, characterized by elevated IgM levels but deficient levels of other immunoglobulin isotypes, as well as defects in cellular immunity. Other disorders linked to IgM include Selective IgM Deficiency, Cold Agglutinin Disease, and Monoclonal Gammopathies.5

Immunoglobulin A is the dominant antibody for mucosal homeostasis in the gastrointestinal, respiratory, and genitourinary tracts. This means they can be found in body secretions such as tears, saliva, respiratory and intestinal secretions, and makes up 50% of the protein in colostrum. IgA gets produced by class switching of Ig and protects against pathogens by neutralization or prevention from binding to the mucosal surfaces.
Researchers are still debating the exact mechanisms and functions of IgA, as there may be large differences between IgA in different mucosal tissues. For instance, a paper by Pabst & Slack (2020) details the disagreement about the relevancy of T cell-dependent versus T cell-independent IgA in both microbiota and infection control.6,7
When in serum, IgA is usually a monomer, but in mucosa, secretory IgA takes a dimeric form with a J-chain and a secretory component. Secretory IgA is produced through the functions of plasma cells producing multimeric IgA and epithelial cells producing pIgR. Which form IgA takes does have interesting consequences, for instance, with how polymeric IgA is more effective than monomeric IgA in preventing Clostridium difficile toxins.
IgA can also be further classified into IgA1 and IgA2. IgA1 has a longer hinge region than IgA2, with a duplicated section of amino acids, making it more susceptible to cleavage from bacterial proteases. This may explain why IgA2 is dominant in many mucosal secretions and the colon, while approximately 90% of total IgA in serum is comprised of IgA1.8

Immunoglobulin D constitutes approximately 0.25% of all serum immunoglobulins in the body, and there is still debate over the specific role for IgD. There is evidence suggesting they may play a part in basophil and mast cell activation to produce antimicrobial factors, as well as determining if antigens will activate B cells.9
In humans, although most mature B cells express both surface IgD and IgM by alternative splicing of preRNA, a small group of mucosal B cells from the nasopharyngeal lymphoid tissue expresses solely IgD. This secreted IgD can be found in circulation, nasopharyngeal, oral and lachrymal secretions, in addition to being on the surface of myeloid innate effector cells, such as basophils, mast cells and monocytes. When IgD is basophil-bound and cross-linked by an antigen, the release of cytokine IL-4 will trigger an increase in IgG production, thus enhancing humoral immunity by the mucosal immune surveillance.10
Moreover, the IgD molecule has a lengthy hinge region between Fab and Fc, which is the likely cause for IgD to be susceptible to proteolysis, although this increases flexibility and thus improves antigen binding. Interestingly, the hinge region also appears to regulate the responsiveness of B cells, as Übelhart et al. (2015) discovered when deleting it resulted in IgD being reactive to monovalent antigens, while transferring the hinge to IgM resulted in responsiveness only to polyvalent antigens.11
Meanwhile, serum IgD is thought to represent an early marker of B-cell activation. Other potential functions of IgD include having a regulatory role, the generation and maintenance of B-cell memory, and as an inducer of TNF-α, IL-1β, and IL-1 receptor antagonist. Furthermore, serum IgD measurement can be important for monitoring of IgD myelomas by measuring the protein concentration of the M spike in serum protein electrophoresis.

Immunoglobulin E makes up the lowest serum concentration of all isotypes, but it is strongly potent, being associated with mediating hypersensitivity and allergic reactions, in addition to having roles in antiparasitic activity, autoimmune processes, and venom protection.
Since IgE is a monomer composed of two epsilon-heavy chains and light chains, it can only bind two antigens, but the structure of their heavy chain C-terminal regions is crucial for the binding to high-affinity cellular receptor Fc-epsilon R1 and low-affinity CD23.12
FcɛRI is expressed on mast cells, basophils, Langerhans cells, and eosinophils, with circulating IgE upregulating FcɛR expression on these cells. This expression and upregulation are what allows the highly potent IgE to be responsible for immediate hypersensitivity reactions, parasitic immunity, enhanced cytokine production, and antigen presentation. This ultimately results in cellular degranulation and the release of vasoactive and pro-inflammatory mediators.13,14
On the other hand, CD23 is mainly expressed on B-cells, T-cells, and antigen-presenting cells, and manages IgE production homeostasis, facilitated antigen presentation, and IgE transportation through airway and gut epithelial cells.
Recently, research into anti-IgE antibodies as therapy for allergy and asthma has been increasing, with antibodies being designed to target free IgE and membrane-bound IgE. As of now, the monoclonal antibody omalizumab is the only licensed anti-IgE therapy available for clinical use in allergic asthma and chronic spontaneous urticaria. Other drugs in development include ligelizumab, which demonstrates improvements to IgE binding, production and basophil activation compared to omalizumab. Furthermore, IgE antibody MOv18 has shown potential for cancer therapy.15
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including HTP Recombinant Antibody Production, Bispecific Antibody Production, Large Scale Antibody Production, and Afucosylated Antibody Expression. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Schroeder, H. W., & Cavacini, L. (2010). Structure and Function of Immunoglobulins. The Journal of Allergy and Clinical Immunology, 125(2 0 2), S41. https://doi.org/10.1016/J.JACI.2009.09.046
Borad, S. G., & Singh, A. K. (2022). Immunoglobulins. Encyclopedia of Dairy Sciences, 894–900. https://doi.org/10.1016/B978-0-12-818766-1.00367-6
Ciobanu, A. M., Dumitru, A. E., Gica, N., Botezatu, R., Peltecu, G., & Panaitescu, A. M. (2020). Benefits and Risks of IgG Transplacental Transfer. Diagnostics, 10(8). https://doi.org/10.3390/DIAGNOSTICS10080583
Schroeder, H. W., & Cavacini, L. (2010). Structure and Function of Immunoglobulins. The Journal of Allergy and Clinical Immunology, 125(2 0 2), S41. https://doi.org/10.1016/J.JACI.2009.09.046
Sathe, A., & Cusick, J. K. (2022). Biochemistry, Immunoglobulin M. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK555995/
Schroeder, H. W., & Cavacini, L. (2010). Structure and Function of Immunoglobulins. The Journal of Allergy and Clinical Immunology, 125(2 0 2), S41. https://doi.org/10.1016/J.JACI.2009.09.046
Pabst, O., & Slack, E. (2019). IgA and the intestinal microbiota: the importance of being specific. Mucosal Immunology 2019 13:1, 13(1), 12–21. https://doi.org/10.1038/s41385-019-0227-4
Stubbe, H., Berdoz, J., Kraehenbuhl, J.-P., & Corthésy, B. (2000). Polymeric IgA is superior to monomeric IgA and IgG carrying the same variable domain in preventing Clostridium difficile toxin A damaging of T84 monolayers. Journal of Immunology (Baltimore, Md. : 1950), 164(4), 1952–1960. https://doi.org/10.4049/JIMMUNOL.164.4.1952
Vladutiu, A. O. (2000). Immunoglobulin D: Properties, Measurement, and Clinical Relevance. Clinical and Diagnostic Laboratory Immunology, 7(2), 131. https://doi.org/10.1128/CDLI.7.2.131-140.2000
Gutzeit, C., Chen, K., & Cerutti, A. (2018). The enigmatic function of IgD: some answers at last. European Journal of Immunology, 48(7), 1101–1113. https://doi.org/10.1002/EJI.201646547
Übelhart, R., Hug, E., Bach, M. P., Wossning, T., Dühren-Von Minden, M., Horn, A. H. C., Tsiantoulas, D., Kometani, K., Kurosaki, T., Binder, C. J., Sticht, H., Nitschke, L., Reth, M., & Jumaa, H. (2015). Responsiveness of B cells is regulated by the hinge region of IgD. Nature Immunology 2015 16:5, 16(5), 534–543. https://doi.org/10.1038/ni.3141
Schroeder, H. W., & Cavacini, L. (2010). Structure and Function of Immunoglobulins. The Journal of Allergy and Clinical Immunology, 125(2 0 2), S41. https://www.jacionline.org/article/S0091-6749(09)01465-1/fulltext
Godwin, L., Sinawe, H., & Crane, J. S. (2022). Biochemistry, Immunoglobulin E. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK541058/
Gasser, P., Tarchevskaya, S. S., Guntern, P., Brigger, D., Ruppli, R., Zbären, N., Kleinboelting, S., Heusser, C., Jardetzky, T. S., & Eggel, A. (2020). The mechanistic and functional profile of the therapeutic anti-IgE antibody ligelizumab differs from omalizumab. Nature Communications 2020 11:1, 11(1), 1–14. https://www.nature.com/articles/s41467-019-13815-w
Spicer, J., Basu, B., Montes, A., Banerji, U., Kristeleit, R., Miller, R., Veal, G. J., Corrigan, C. J., Till, S. J., Figini, M., Canevari, S., Barton, C., Jones, P., Mellor, S., Carroll, S., Selkirk, C., Nintos, G., Kwatra, V., Funingana, I. G., … Karagiannis, S. N. (2023). Safety and anti-tumour activity of the IgE antibody MOv18 in patients with advanced solid tumours expressing folate receptor-alpha: a phase I trial. Nature Communications 2023 14:1, 14(1), 1–11. https://www.nature.com/articles/s41467-023-39679-9
For an antibody candidate, strong target binding is only part of the path toward……
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
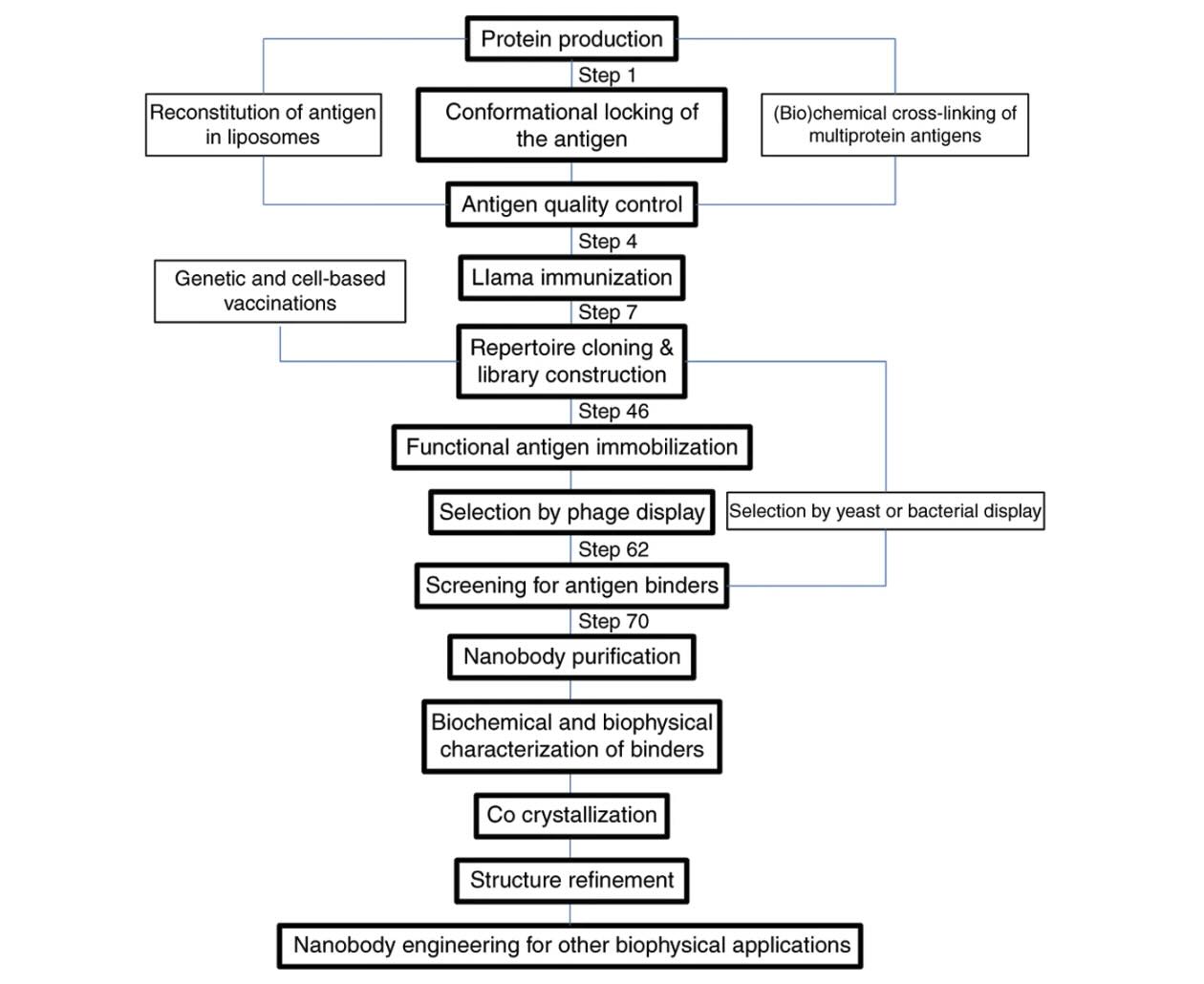
Explore how VHH antibodies stabilize protein conformations for crystallography, ……