Antibody-drug conjugates (ADCs) have transformed cancer therapy by selectively delivering cytotoxic agents to tumor cells. Building on this approach, immune-stimulating antibody conjugates (ISACs) introduce a novel strategy that not only targets tumors but also activates the immune system. ISACs conjugate tumor-targeting monoclonal antibodies (mAbs) with innate immune agonists, facilitating localized immune activation within the tumor microenvironment (TME). This dual mechanism enhances both innate and adaptive immune responses, potentially converting immunologically "cold" tumors into "hot" tumors, which are more responsive to immunotherapy.
Despite their promise, ISACs remain in early clinical development, with multiple candidates encountering setbacks. Key challenges include balancing immune activation with toxicity, optimizing pharmacokinetics, and refining conjugation strategies to maximize efficacy while minimizing adverse effects.
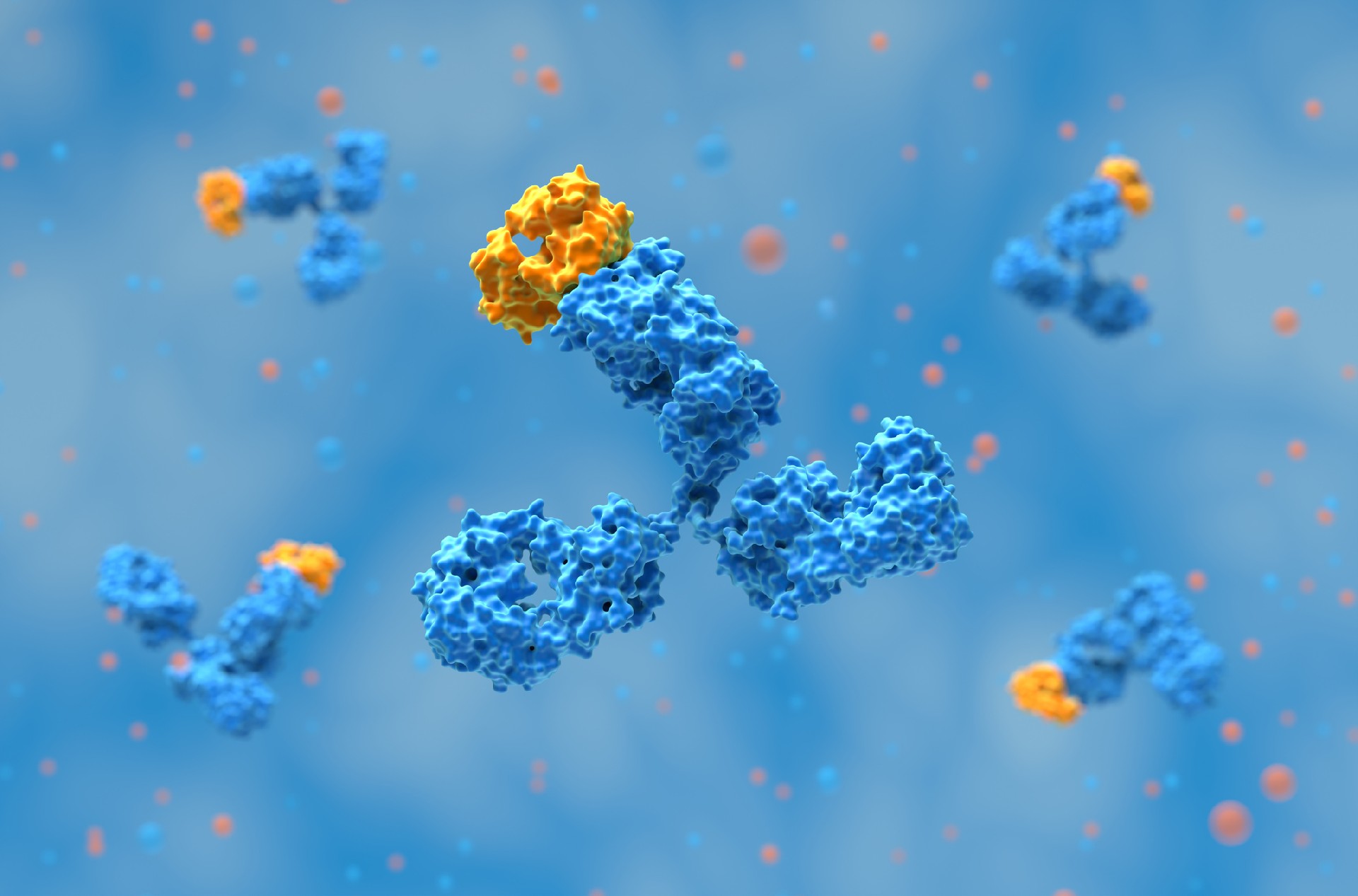
The antibody component of ISACs plays a crucial role in tumor targeting and immune activation. Most ISACs use monoclonal antibodies similar to those found in ADCs, with IgG1 being the predominant subclass due to its strong Fcγ receptor (FcγR) binding capacity. This enhances antibody-dependent cellular phagocytosis (ADCP) and antibody-dependent cellular cytotoxicity (ADCC), recruiting immune effector cells for tumor destruction.
Antibody selection criteria include:
Target Specificity: The antigen should be highly expressed in tumors and minimally present in healthy tissues to prevent off-target effects.
Internalization Rate: While high internalization is desirable for ADCs, ISACs rely on surface binding to facilitate immune activation.
Binding Affinity: Moderate affinity may be preferable, as excessively strong binding can result in rapid internalization and degradation, limiting immune activation within the TME.
Commonly used antibodies in ISACs target HER2, PD-1, CTLA-4, EGFR, and CD20. Trastuzumab-based ISACs, such as BDC-1001, have shown promising preclinical results but require further clinical validation.
The linker is a critical component in ISAC design, ensuring the stable attachment of immune agonists to the antibody. Unlike ADCs, which often use cleavable linkers to release cytotoxic payloads inside tumor cells, ISACs primarily employ non-cleavable linkers to retain immune agonists on the antibody for optimal immune activation.
Key considerations for linker design include:
Chemical Stability: The linker must remain intact in circulation to prevent systemic immune activation.
Hydrophilicity: Optimal hydrophilicity prevents aggregation and enhances pharmacokinetics.
Payload Release Mechanism: A controlled release mechanism can enhance efficacy and safety by reducing systemic toxicity.

The immune-stimulating payload is the defining feature of ISACs. These payloads typically include agonists of toll-like receptors (TLRs), stimulator of interferon genes (STING), and other innate immune modulators.
TLR7/8 Agonists: Activate dendritic cells and macrophages, bridging innate and adaptive immunity.
TLR9 Agonists: Promote antigen presentation and cytokine production.
Examples: SBT6050, BDC-1001 (TLR7/8 agonist conjugated to trastuzumab).
Activate type I interferon pathways to enhance anti-tumor immunity.
Examples: XMT-2056, currently in preclinical development.
While these agonists show promise, their systemic administration has been linked to severe immune-related toxicities, including cytokine release syndrome (CRS). Strategies to mitigate these risks include dose adjustments, alternative administration routes, and molecular modifications to optimize pharmacokinetics.
Related: ADC Payloads: Expanding Beyond Microtubules and DNA-Damaging Agents
BDC-1001, a HER2-targeting immune-stimulating antibody conjugate (ISAC) developed by Bolt Biotherapeutics, is currently in Phase II clinical trials. This conjugate consists of a trastuzumab biosimilar linked to a TLR7/8 agonist via a non-cleavable linker. Its mechanism of action involves three key steps: tumor targeting, where the trastuzumab component binds to HER2-expressing tumor cells; innate immune activation, in which Fc-mediated uptake by antigen-presenting cells (APCs) leads to TLR7/8 activation; and the adaptive immune response, where activated APCs prime T cells to enhance tumor-specific immunity. Preclinical studies demonstrated robust tumor regression and immune memory formation, while Phase I/II trials showed mixed results, with some patients achieving stable disease but overall limited response rates. Several challenges emerged in clinical trials, including dose escalation limitations, as higher doses were necessary for efficacy but led to increased toxicity; limited internalization, since ISACs do not rely on intracellular delivery like antibody-drug conjugates (ADCs), affecting pharmacokinetics; and a trade-off between agonist potency and safety, where high-potency TLR agonists triggered excessive cytokine release, while lower-potency agonists failed to achieve sufficient immune activation. This eventually resulted in the discontinuation of development.

Several biotech companies are actively developing ISACs, including:
SBT6050 (Silverback Therapeutics): HER2-targeted ISAC with a TLR8 agonist, halted due to dose-limiting toxicity.
XMT-2056 (Mersana Therapeutics): A STING-agonist ISAC with ongoing Phase 1 studies.
ISACs Targeting PD-L1 and CEA: Emerging candidates showing preclinical efficacy.
Despite early failures, ISACs remain a promising therapeutic approach. Addressing safety concerns and optimizing drug-to-antibody ratios (DARs) could improve clinical outcomes.
Related: Antibody-Drug Conjugates (ADCs) and Drug–Antibody Ratio (DAR)
Modulating Drug-to-Antibody Ratio (DAR):
A higher DAR enhances potency but increases hydrophobicity, potentially leading to aggregation and faster clearance.
An optimized DAR (typically 2–4) balances efficacy with pharmacokinetics.
Alternative Immune Modulators:
Using less potent but safer immune agonists (e.g., BTK inhibitors) could reduce systemic toxicity while maintaining immune activation.
Bispecific and Multispecific ISACs:
Dual-target ISACs could enhance tumor specificity and reduce off-target effects.
Example: Combining HER2 and PD-L1 targeting to broaden immune activation.
Combination Therapy Approaches:
ISACs could be combined with immune checkpoint inhibitors (e.g., anti-PD-1) to enhance T cell responses.
Synergistic effects with chemotherapy or radiation could be explored.
While ISACs represent a novel class of immunotherapeutic agents, their clinical translation remains challenging. The failures of early candidates highlight the need for optimized agonist selection, refined linker chemistry, and improved dosing strategies. Nevertheless, the ability of ISACs to harness both innate and adaptive immunity provides a unique therapeutic advantage over traditional ADCs.
Future developments will likely focus on:
Safer and More Selective Immune Agonists to minimize systemic toxicity.
Improved Conjugation Strategies to optimize drug stability and pharmacokinetics.
Personalized Treatment Approaches based on tumor immune profiling.
With continued research, ISACs have the potential to redefine targeted immunotherapy, bridging the gap between ADCs and immune checkpoint inhibitors in cancer treatment.
Related: Antibody-Drug Conjugates with In Vivo Research
References:
Fu, C., Tong, W., Yu, L., Miao, Y., Wei, Q., Yu, Z., Chen, B., & Wei, M. (2024). When will the immune-stimulating antibody conjugates (ISACs) be transferred from bench to bedside? Pharmacological Research, 203, 107160. https://doi.org/10.1016/j.phrs.2024.107160
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……
Post-translational modifications (PTMs) are chemical or structural changes made ……
Research recap on Antibody Engineering & Therapeutics Europe 2026. Antibody inno……