In the 1990s, a significant breakthrough changed the landscape of inflammatory disease treatment: the development of the anti-TNF monoclonal antibody cA2, later known as infliximab. Dr. Marc Feldmann and Dr. Ravinder Maini's work demonstrated that infliximab could effectively mitigate symptoms in patients suffering from rheumatoid arthritis (RA), a progressive autoimmune disorder characterized by chronic joint inflammation and severe pain.1
Infliximab (marketed as Remicade) was first approved by the U.S. Food and Drug Administration (FDA) in 1998. It was initially approved for the treatment of Crohn's disease and has since received additional approvals for conditions like rheumatoid arthritis, ulcerative colitis, psoriatic arthritis, ankylosing spondylitis, and plaque psoriasis.
The Role of TNF in Autoimmune Diseases
Tumor necrosis factor (TNF) is a cytokine integral to immune signaling, involved in systemic inflammation and the activation of immune cells. While TNF plays a crucial role in defending against infections, excessive TNF production is harmful, triggering inflammation that attacks the body's own tissues. In diseases like rheumatoid arthritis, TNF is overexpressed, leading to chronic joint inflammation and degradation.
By binding to TNF, infliximab disrupts this inflammatory cycle, helping to reduce symptoms of joint pain, swelling, and damage. The identification of TNF as a therapeutic target was a critical insight that transformed approaches to managing not only RA but other TNF-mediated diseases, including Crohn's disease and psoriasis. Blocking TNF activity has since become a cornerstone in treating various autoimmune conditions.
Related: Therapeutic targets - Autoimmune Diseases
Infliximab Mechanisms of Action
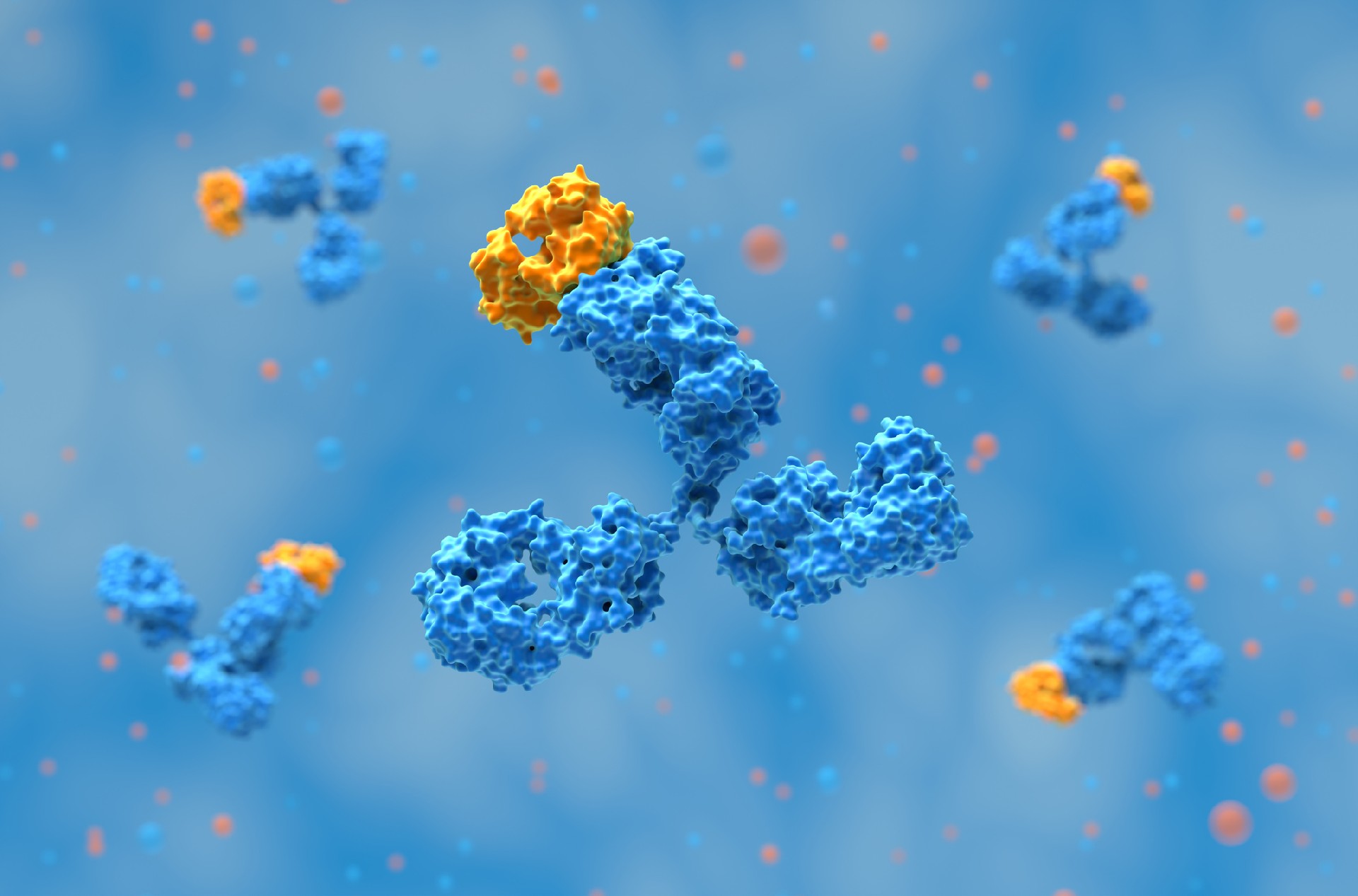
Infliximab, a chimeric monoclonal antibody, is designed to specifically bind to TNF-α, a dominant form of TNF in inflammatory responses. Once bound, infliximab neutralizes TNF-α, preventing it from interacting with TNF receptors on cell surfaces. This halts the cascade of pro-inflammatory signals that would otherwise lead to the activation and proliferation of immune cells that attack healthy tissue in RA patients.
Another significant mechanism is infliximab’s ability to induce apoptosis (programmed cell death) in certain immune cells, such as activated T-cells, which are present in high numbers in the inflamed joints of RA patients. By reducing these immune cells, infliximab minimizes the autoimmune attack on joint tissue, helping to control the symptoms and slow the progression of RA.
The effectiveness of infliximab demonstrated the viability of monoclonal antibody therapies in targeting specific molecules involved in disease pathology. This targeted approach contrasts with traditional treatments like corticosteroids, which suppress the immune system more broadly and often carry significant side effects. Infliximab's focused mechanism provides therapeutic efficacy with a more manageable safety profile, although it is not without side effects.
Clinical Success and Challenges of Infliximab in Rheumatoid Arthritis
The landmark clinical trials on infliximab showed remarkable efficacy in reducing RA symptoms. Many patients experienced significant relief from pain, improved joint function, and reduced disease progression. These results were significant enough to secure regulatory approval, with infliximab becoming the first anti-TNF therapy for rheumatoid arthritis.
However, the adoption of infliximab also highlighted challenges. Some patients developed resistance over time, while others experienced adverse effects, such as infections and infusion reactions. Because infliximab is a chimeric antibody (part human and part mouse), patients could sometimes develop anti-drug antibodies (ADAs) that reduce the therapy’s effectiveness.2
Related: Muronomab: The First Approved Monoclonal Antibody
Ongoing Research for Anti-TNF Therapies
Despite the success of infliximab and other anti-TNF therapies, research is ongoing to address limitations, such as loss of efficacy in some patients and adverse immune responses. Current strategies include developing combination therapies that target multiple immune pathways, which may provide sustained benefits for patients who do not respond to TNF inhibitors alone.
Another promising area is the development of biosimilars to infliximab, which offer a more cost-effective alternative to the original drug. Biosimilars have made these treatments more accessible, particularly in countries with limited healthcare resources. The introduction of biosimilars has also heightened the focus on quality control in antibody production, emphasizing the need for reliable and scalable antibody expression systems to ensure that biosimilars meet the efficacy and safety standards of their reference products.
Biointron’s catalog products for in vivo research can be found at Abinvivo, where we have a wide range of Benchmark Positive Antibodies, Isotype Negative Antibodies, Anti-Mouse Antibodies, Bispecific Antibodies, and Antibody-Drug Conjugates, including:
V6 Anti-Human TNFA (Infliximab)-B21631112
Contact us to find out more at info@biointron.com or +86 400-828-8830 / +1(732)790-8340.
Elliott, M. J., Maini, R. N., Feldmann, M., Long-Fox, A., Charles, P., Katsikis, P., Brennan, F. M., Walker, J., Bijl, H., Ghrayeb, J., & Woody, J. N. (1993). Treatment of rheumatoid arthritis with chimeric monoclonal antibodies to tumor necrosis factor α. Arthritis & Rheumatism, 36(12), 1681-1690. https://doi.org/10.1002/art.1780361206
Brun, M. K., Goll, G. L., Jørgensen, K. K., Sexton, J., Gehin, J. E., Sandanger, Ø., Olsen, I. C., Klaasen, R. A., Warren, D. J., Mørk, C., Kvien, T. K., Jahnsen, J., Bolstad, N., Haavardsholm, E. A., & Syversen, S. W. (2022). Risk factors for anti-drug antibody formation to infliximab: Secondary analyses of a randomised controlled trial. Journal of internal medicine, 292(3), 477–491. https://doi.org/10.1111/joim.13495
Two popular topics discussed at the 2026 BIO International Convention were devel……
AI is changing antibody discovery, but model performance depends on the quality ……
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……