Personalized medicine, also known as individualized medicine, is a medical approach that tailors treatment to the individual characteristics of each patient. Precision medicine is similar but stratifies therapies for subgroups of patients who possess, for instance, a genetic variant of interest. It takes into account both your genetic and environmental factors for the development of diagnostic, prognostic, and therapeutic strategies. This personalization allows it to be particularly applicable to cancer, as tumors tend to arise from genetic variants.1,2
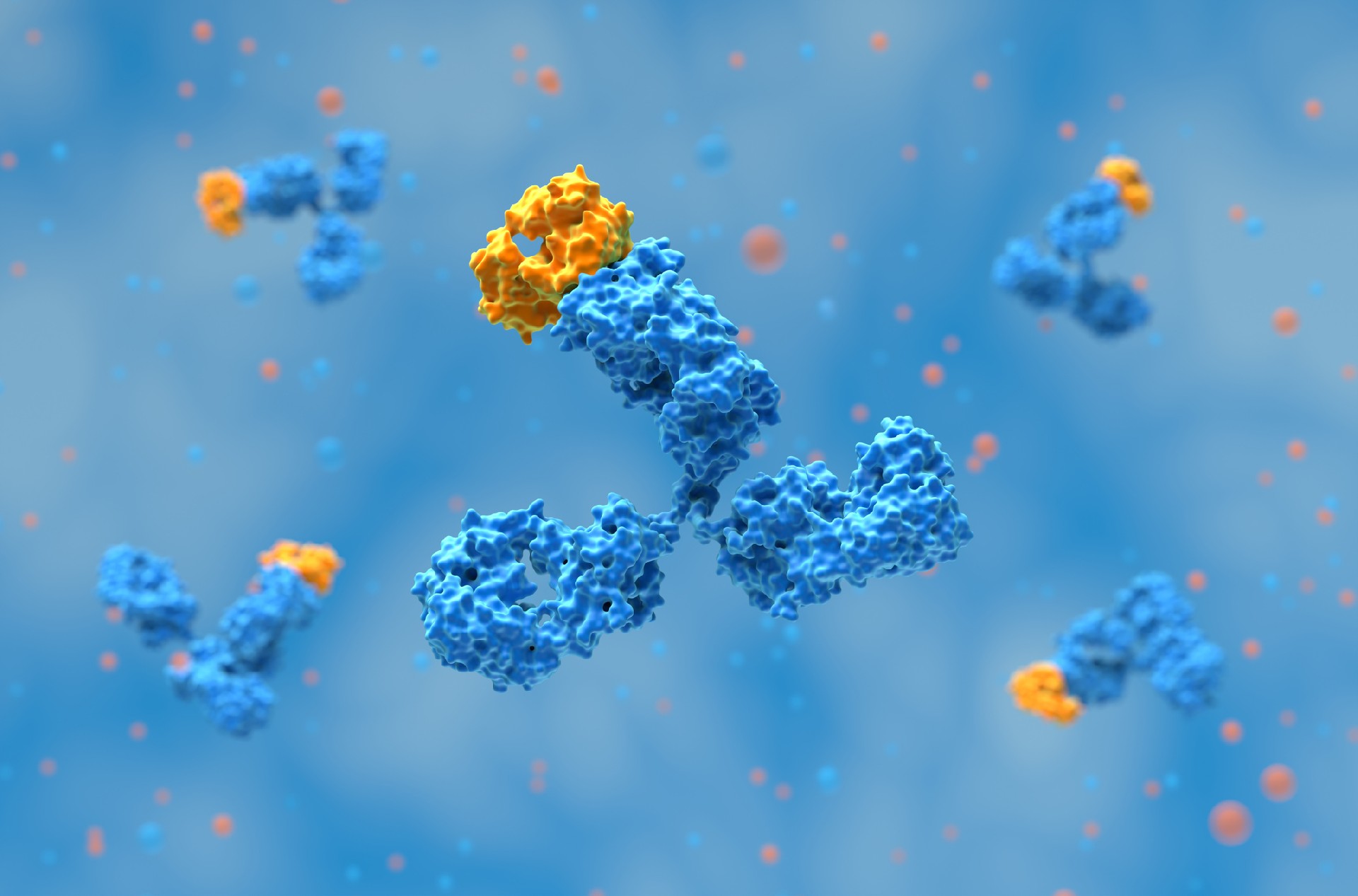
Antibody drugs are suitable as personalized medicine due to their high specificity. Monoclonal antibodies (mAbs) can be designed to target specific antigens and have been indicated for several tumors, in addition to being used in diagnostic tools to identify the source of a tumor. mAbs may be associated to biomarkers such as HER2, KRAS, or PD-L1, which are molecules in the body that can be used to signal normal or abnormal activity in a patient.
Currently, target prioritization is still a challenge for personalization, as there are relatively few biomarkers. Those that have been reported for mAb drugs, are typically the same ones. Garattini and Padula (2019) report a tendency to treat cancer tumors with different sites of origin with combination therapies instead of developing therapies encompassing a single cancer.
Another area where mAbs can be useful as personalized medicine is inflammatory bowel disease (IBD). Traditional therapies for IBDs such as Crohn's disease and ulcerative colitis are based on aminosalicylates, antimetabolites, and immunosuppressants. However, therapeutic effectiveness varies in patients, leading to a search for more personalized treatments, such as mAbs, which have ideal pharmacokinetic characteristics. This includes a relatively small volume of distribution, a clearance depending on many activities, a minimal renal excretion, and the presence of antidrug antibodies.3
Besides mAbs, antibody-drug conjugates (ADCs) represent a fast-growing area of therapeutics. ADCs combine the specificity of mAbs with a cytotoxic (cell-killing) payload through covalent bonds. In cancer, this approach aims to deliver chemotherapy directly to cancer cells via specific binding to cell surface receptors on a solid tumor, while minimizing damage to normal, healthy cells. Since the level of target expression is a main factor in anticipating the ADC’s benefit for patients, establishing a patient selection strategy is important for a personalized approach.4
At Biointron, we are dedicated to accelerating your antibody discovery, optimization, and production needs. Our team of experts can provide customized solutions that meet your specific research needs. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Garattini, L., & Padula, A. (2019). Precision medicine and monoclonal antibodies: Breach of promise? Croatian Medical Journal, 60(3), 284-289. https://doi.org/10.3325/cmj.2019.60.284
Jain, K. K. (2021). Personalized Immuno-Oncology. Medical Principles and Practice, 30(1), 1-16. https://doi.org/10.1159/000511107
Di Paolo, A., & Luci, G. (2021). Personalized Medicine of Monoclonal Antibodies in Inflammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and Beyond. Frontiers in Pharmacology, 11, 610806. https://doi.org/10.3389/fphar.2020.610806
Gogia, P., Ashraf, H., Bhasin, S., & Xu, Y. (2023). Antibody–Drug Conjugates: A Review of Approved Drugs and Their Clinical Level of Evidence. Cancers, 15(15). https://doi.org/10.3390/cancers15153886
Two popular topics discussed at the 2026 BIO International Convention were devel……
AI is changing antibody discovery, but model performance depends on the quality ……
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……