For more than 30 years, antibody drug development has transformed the landscape of immunotherapy, treating various diseases from cancer to autoimmune diseases. The use of therapeutic monoclonal antibodies (mAbs) began after the groundbreaking development of the hybridoma technique by Kohler and Milstein in 1975, with further development into humanization approaches over the next decade.
As of now, more than 100 therapeutic antibodies have received approval from the FDA, with an exponential increase in approvals. Besides mAbs, which are ideal as cancer therapeutics due to their highly specific binding to target antigens and cytotoxicity effects, other antibody formats such as VHHs, antibody fragments, bispecific antibodies, and non-IgG scaffold proteins, have been successfully developed. Furthermore, antibody derivatives such as antibody-drug conjugates (ADCs) and immunocytokines are becoming much more widely studied.
Monoclonal Antibodies in Cancer Therapy
Monoclonal antibodies (mAbs) can selectively target cancer cell antigens. Their highly specific binding allows for precision targeting, reducing damage to healthy tissues while delivering potent cytotoxic effects to cancer cells. This specificity minimizes side effects compared to chemotherapy and radiation, which indiscriminately damage both cancerous and healthy cells.
Antibody-Dependent Cellular Cytotoxicity (ADCC): Many therapeutic mAbs function by recruiting immune cells, such as natural killer (NK) cells, to destroy tumor cells. Antibodies like rituximab, which target the CD20 protein on B cells, effectively trigger ADCC and have revolutionized treatments for lymphomas and leukemias.
Immune Checkpoint Inhibitors: These mAbs work by blocking inhibitory pathways that cancer cells use to evade the immune system. Examples include anti-PD-1 (programmed cell death-1) and anti-CTLA-4 (cytotoxic T-lymphocyte-associated protein 4) antibodies, which have shown remarkable success in cancers such as melanoma, lung cancer, and renal cell carcinoma. By reactivating the immune system, these antibodies enable a stronger and more sustained attack against tumors.
Targeted Delivery of Cytotoxic Agents: Some mAbs are conjugated with cytotoxic drugs, forming Antibody-Drug Conjugates (ADCs). ADCs selectively deliver chemotherapy agents directly to cancer cells, sparing healthy cells from exposure. This targeted approach allows for higher concentrations of the cytotoxic drug at the tumor site, improving efficacy while reducing systemic toxicity.
Beyond Monoclonal Antibodies: Expanding Antibody Formats
While monoclonal antibodies form the majority of antibody-based therapeutics, there is a growing interest in other formats.
VHHs (single-domain antibodies): Derived from camelid antibodies and consisting of only the variable region of the heavy chain, their small size allows for better tissue penetration, making them ideal for targeting antigens in dense or hard-to-reach tissues, such as solid tumors.
Antibody Fragments: Similarly, antibody fragments like Fab (fragment antigen-binding) and scFv (single-chain variable fragment) can be less likely to trigger immune responses, and they can access epitopes that are inaccessible to larger antibodies.
Bispecific Antibodies: Bispecific antibodies are engineered to bind two different antigens simultaneously. This dual-targeting approach enhances therapeutic efficacy and can bridge immune cells to cancer cells, promoting more efficient killing of tumor cells. Blinatumomab, a bispecific T-cell engager (BiTE), is a notable example used in the treatment of acute lymphoblastic leukemia.
Antibody-Drug Conjugates (ADCs): Precision Targeting with Potent Cytotoxicity
Antibody-Drug Conjugates (ADCs) combine the specificity of antibodies with the potency of small-molecule cytotoxins.
Structure: ADCs consist of three key components: a monoclonal antibody that targets a specific antigen, a cytotoxic drug, and a linker that connects the drug to the antibody. The choice of linker is crucial, as it must remain stable in circulation but release the drug once the ADC reaches the target cells.
Mechanism of Action: Once the ADC binds to the target antigen on cancer cells, it is internalized into the cell, where the cytotoxic drug is released. The released drug then kills the cancer cells, often by disrupting DNA or inhibiting key cellular processes.
Clinical Successes: ADCs like trastuzumab emtansine (T-DM1) have shown significant success in treating HER2-positive breast cancer. This ADC combines the HER2-targeting capabilities of trastuzumab with the cytotoxic agent emtansine, providing a dual mechanism for attacking cancer cells.
Related: Antibody-Drug Conjugates: A Brief
References:
Jin, S., Sun, Y., Liang, X., Gu, X., Ning, J., Xu, Y., Chen, S., & Pan, L. (2022). Emerging new therapeutic antibody derivatives for cancer treatment. Signal Transduction and Targeted Therapy, 7(1), 1-28. https://doi.org/10.1038/s41392-021-00868-x
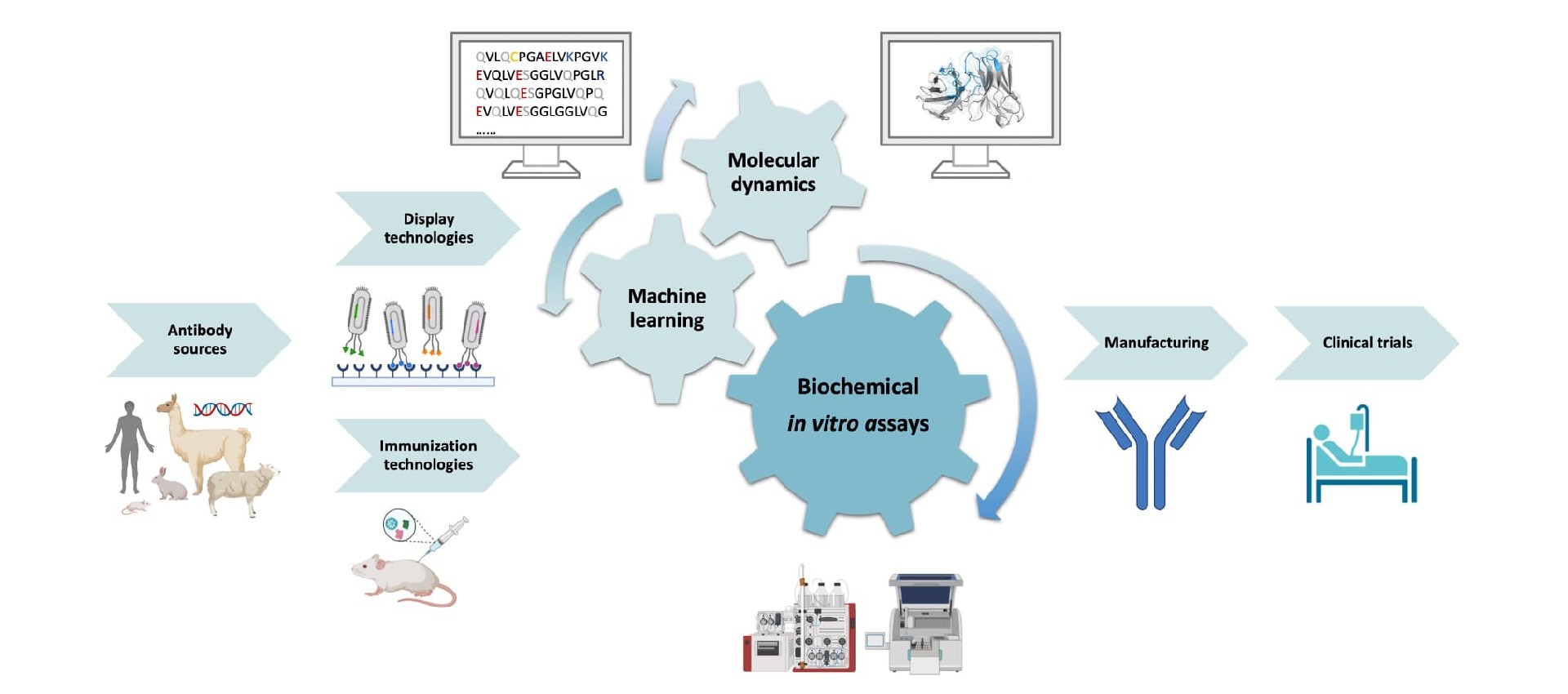
For an antibody candidate, strong target binding is only part of the path toward……
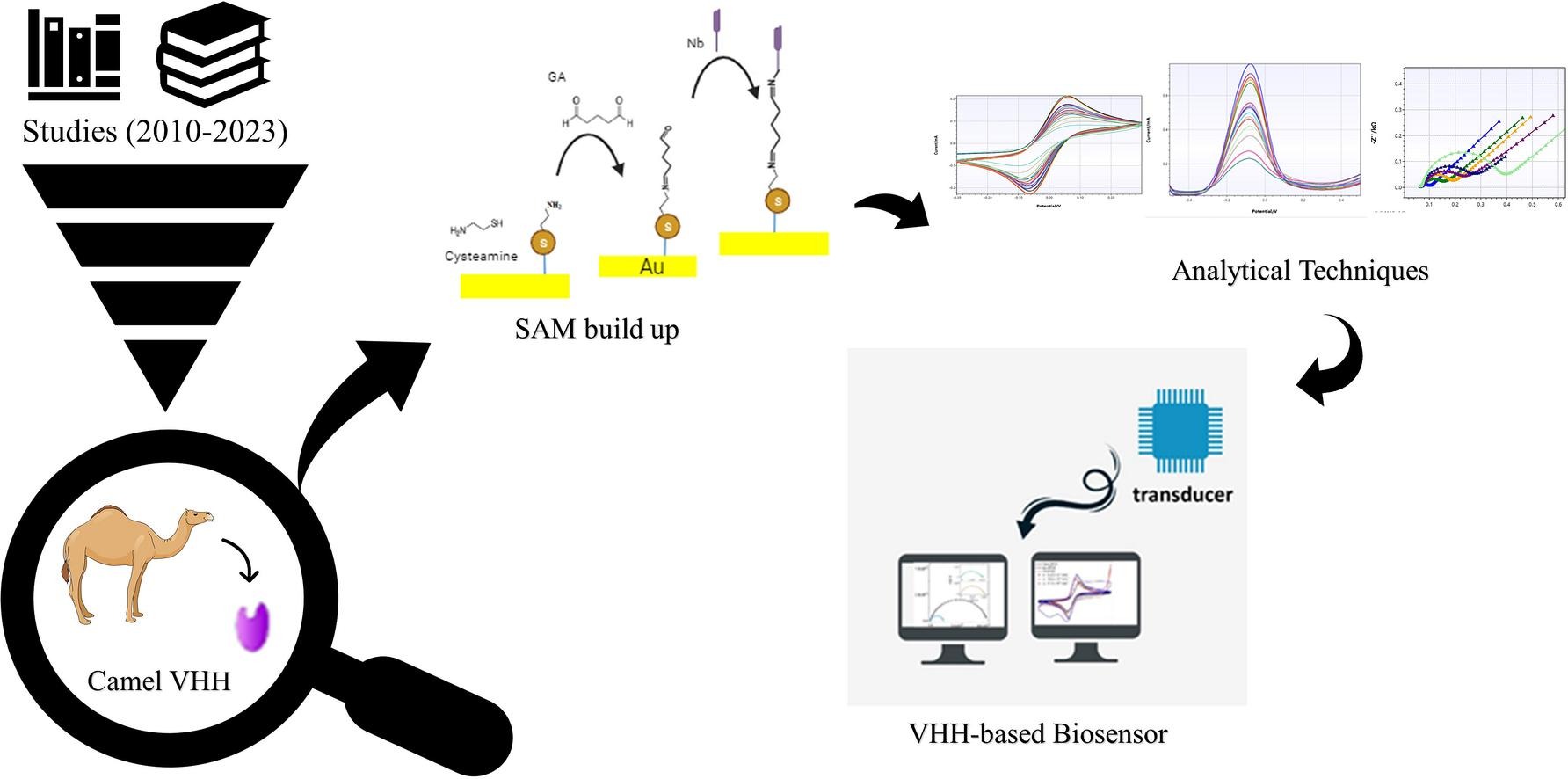
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
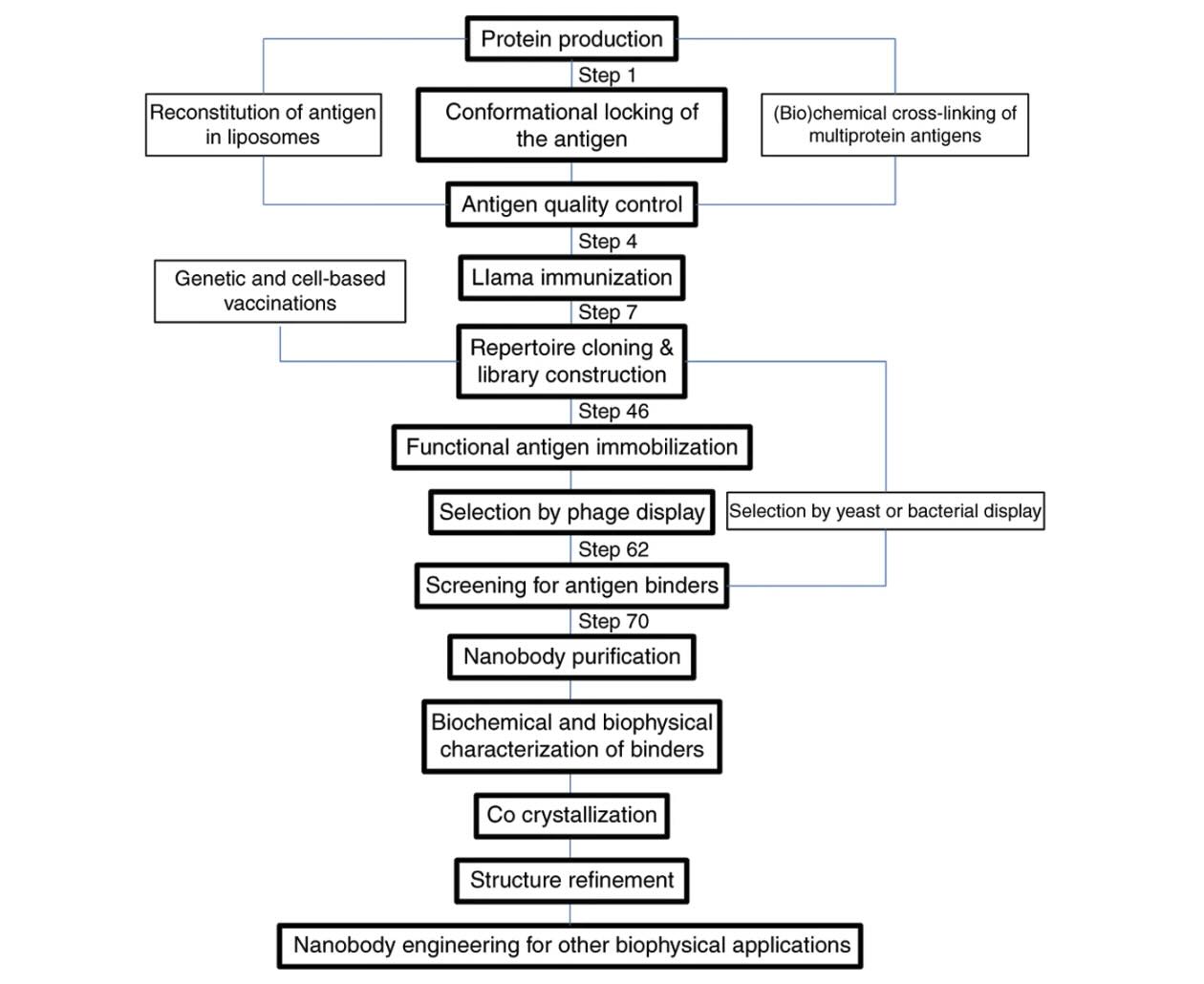
Explore how VHH antibodies stabilize protein conformations for crystallography, ……