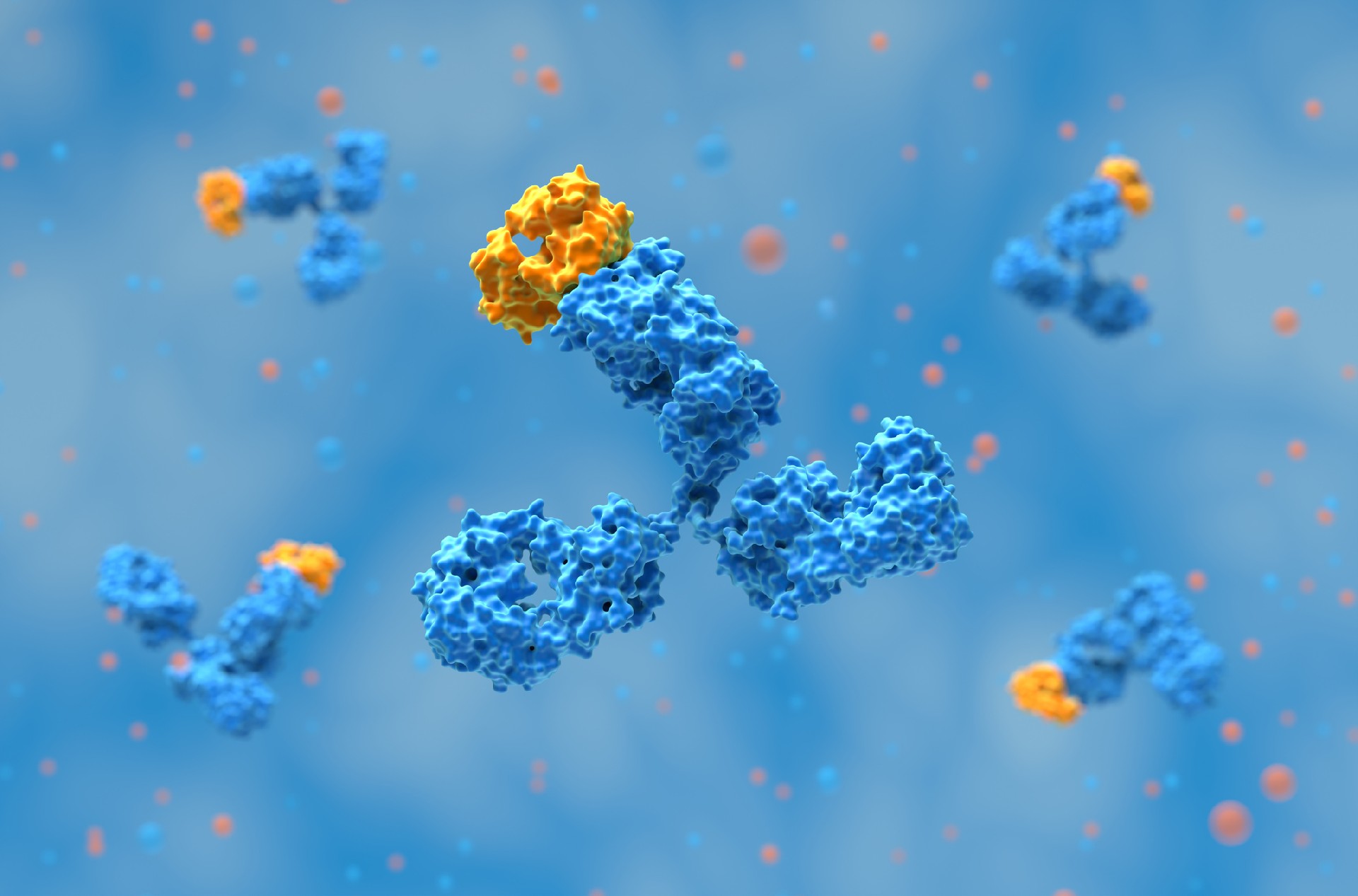
The immune system plays a critical role in identifying and eliminating cancer cells. However, tumors can evade immune detection by exploiting immune checkpoints, which are molecular brakes that prevent excessive immune activation. One of the key checkpoints is cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), which downregulates T-cell activity. Ipilimumab, sold under the brand name Yervoy, is a monoclonal antibody targeting CTLA-4, was the first immune checkpoint inhibitor to receive FDA approval, marking a breakthrough in cancer immunotherapy. Since its approval for metastatic melanoma in 2011, ipilimumab has been investigated for multiple malignancies and has contributed to the expansion of immune checkpoint blockade therapies.1
The concept of using the immune system to fight cancer, known as cancer immunotherapy, has long intrigued scientists. Despite early successes in mouse models, translating these findings to humans proved challenging, leading many researchers and biotechnology companies to abandon immunotherapy approaches by the 1990s. However, Dr. James P. Allison, then at the UC Berkeley Cancer Research Laboratory, remained committed to this idea. His research focused on CTLA-4, a molecule found on T cells that functions as an immune checkpoint, preventing excessive immune activation. In a landmark 1996 Science paper, Allison and his colleagues demonstrated that blocking CTLA-4 with antibodies enabled T cells to mount a stronger antitumor response, successfully eliminating tumors in mouse models. This pioneering discovery laid the foundation for checkpoint blockade as a therapeutic strategy in oncology.2
Related: Pivotal Moments in Oncology Antibody Drug Development
Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) is an essential immune checkpoint receptor expressed on T cells. It serves as a negative regulator of immune responses, helping to maintain immune homeostasis and prevent excessive immune activation. CTLA-4 competes with the co-stimulatory receptor CD28 for binding to the B7 ligands, CD80 and CD86, on antigen-presenting cells (APCs). Unlike CD28, which promotes T-cell activation, CTLA-4 has a much higher affinity for B7 molecules and functions to dampen immune responses. This regulatory mechanism is crucial for preventing autoimmunity but is also exploited by tumors to evade immune detection.
Checkpoint inhibitors, such as ipilimumab, work by blocking CTLA-4, effectively releasing the “brakes” on the immune system and allowing T cells to mount stronger antitumor responses. This has been particularly effective in treating metastatic melanoma and other cancers. However, because CTLA-4 plays a fundamental role in immune tolerance, its inhibition can also lead to immune-related toxicities, including inflammation of the gastrointestinal tract, skin, liver, and endocrine organs.
CTLA-4 is expressed on both CD4+ and CD8+ T cells, but its role is particularly prominent in regulatory T cells (Tregs), where it contributes to immune suppression. While CD28 is constitutively expressed on the plasma membrane, CTLA-4 is predominantly localized in intracellular vesicles and is rapidly internalized through clathrin-mediated endocytosis. This results in only a small fraction of CTLA-4 being present on the cell surface at any given time, with dynamic recycling between intracellular compartments and the plasma membrane. The AP2 and LRBA (lipopolysaccharide-responsive and beige-like anchor protein) complexes regulate CTLA-4 trafficking, influencing its availability for ligand binding.
One of the key mechanisms by which CTLA-4 regulates immune responses is trans-endocytosis, in which CTLA-4 actively removes CD80 and CD86 from APCs. By depleting these ligands, CTLA-4 reduces the ability of APCs to provide co-stimulation through CD28, thereby limiting T-cell activation. This process plays a significant role in maintaining immune tolerance and suppressing excessive immune responses.3

Ipilimumab works by blocking CTLA-4, a critical negative regulator of T-cell activation. Under normal conditions, T-cell activation requires two signals:
The binding of the T-cell receptor (TCR) to an antigen presented by major histocompatibility complexes (MHC) on antigen-presenting cells (APCs).
The interaction between CD28 on T cells and CD80/CD86 on APCs, which provides a co-stimulatory signal necessary for full activation.
Once T cells are activated, CTLA-4 is upregulated and competes with CD28 for binding to CD80/CD86 with higher affinity, leading to inhibition of T-cell activation. By blocking CTLA-4, ipilimumab prevents this inhibitory signal, sustaining T-cell activation and enhancing the immune response against tumors. This results in a robust antitumor effect, allowing T cells to target and destroy malignant cells more effectively.
Related: Monoclonal Antibodies: Evolution, Therapeutic Applications, and Future Directions

Ipilimumab received FDA approval in March 2011 for the treatment of unresectable or metastatic melanoma, making it the first immune checkpoint inhibitor approved for cancer therapy. Since then, its indications have expanded to several malignancies, including:
Renal cell carcinoma (RCC) – Approved in combination with nivolumab for advanced RCC.
Colorectal cancer (CRC) – Approved for microsatellite instability-high (MSI-H)/mismatch repair deficient (dMMR) CRC that has progressed after chemotherapy.
Hepatocellular carcinoma (HCC) – Approved in combination with nivolumab for patients previously treated with sorafenib.
Ongoing clinical trials are investigating ipilimumab in other cancers, including pancreatic and gallbladder tumors, as well as various genitourinary malignancies.
Before the advent of immune checkpoint inhibitors, the prognosis for metastatic melanoma was poor, with limited treatment options. The introduction of ipilimumab revolutionized melanoma treatment by significantly improving survival outcomes. Clinical trials demonstrated long-term durable responses, with some patients achieving extended survival beyond five years—an unprecedented outcome in advanced melanoma at the time.
Combination therapies have further enhanced its efficacy. Ipilimumab plus nivolumab (anti-PD-1 antibody) has become a standard treatment for advanced melanoma, demonstrating superior response rates compared to ipilimumab alone. The combination capitalizes on dual checkpoint blockade, enhancing both the activation and persistence of tumor-fighting T cells.
Following his breakthrough at UC Berkeley, Dr. Allison continued his research at Memorial Sloan Kettering Cancer Center and later at MD Anderson Cancer Center. Despite early skepticism, pharmaceutical company Bristol Myers Squibb recognized the potential of CTLA-4 blockade and pursued the clinical development of ipilimumab (branded as Yervoy). The first Phase III clinical trial, published in 2010 in the New England Journal of Medicine, demonstrated that ipilimumab significantly improved survival in patients with metastatic melanoma, a disease with historically poor prognosis. Importantly, a subset of patients experienced long-lasting remissions, with some achieving apparent cures. This was a breakthrough in oncology, as it showed that checkpoint inhibitors could provide durable responses, unlike conventional chemotherapy, where resistance often develops over time.

As an immune checkpoint inhibitor, ipilimumab enhances T-cell activation, which can lead to immune-related adverse events (irAEs). These toxicities occur because an overactive immune system may attack normal tissues, causing inflammation in various organ systems.
Gastrointestinal: Diarrhea, colitis, and severe enterocolitis, which may lead to intestinal perforation.
Skin: Pruritic rash, Stevens-Johnson syndrome, and toxic epidermal necrolysis.
Endocrine: Hypophysitis, adrenal insufficiency, hypo- and hyperthyroidism.
Liver: Hepatitis with elevated liver enzymes.
Neurological: Peripheral neuropathy, Guillain-Barré syndrome, and encephalitis.
Ocular: Uveitis and conjunctivitis.
Renal and Pulmonary: Nephritis and pneumonitis.
Most immune-related toxicities appear within the first 12 weeks of treatment and resolve over 3 to 4 months with appropriate management. Mild toxicities can be managed with supportive care, including antidiarrheals (e.g., loperamide) and antihistamines for rashes. Moderate to severe toxicities often require systemic corticosteroids, and in some cases, additional immunosuppressants like infliximab may be needed. Severe adverse events may necessitate treatment discontinuation.
Half-life: 15.4 days, allowing for intermittent dosing.
Metabolism: Primarily via the reticuloendothelial system, with minimal involvement of the CYP450 enzyme system.
Dosing: Typically 3 mg/kg every three weeks for four cycles in melanoma, with alternative regimens in combination therapies.
Ipilimumab’s approval paved the way for immune checkpoint inhibitors targeting PD-1 and PD-L1, such as nivolumab and pembrolizumab, which have since become standard treatments for various cancers. The success of ipilimumab also led to the 2018 Nobel Prize in Physiology or Medicine, awarded to Dr. James Allison for his pioneering work on CTLA-4 inhibition.
The future of CTLA-4 blockade is evolving with next-generation bispecific antibodies, dual checkpoint inhibitors, and personalized immunotherapy approaches that tailor treatments based on individual tumor characteristics. Research is also focusing on optimizing the balance between efficacy and toxicity to improve patient outcomes while minimizing immune-related complications. The success of Yervoy inspired the development of next-generation checkpoint inhibitors, including anti-PD-1 and anti-PD-L1 antibodies such as nivolumab and pembrolizumab, which have since become standard treatments in multiple cancers.

Ipilimumab marked a paradigm shift in oncology by proving that immune checkpoint blockade could produce durable responses in cancer. As the first FDA-approved checkpoint inhibitor, it laid the foundation for a new era of immunotherapy. While challenges remain in managing its immune-related toxicities, ongoing research and combination strategies continue to expand its role in cancer treatment. The development of checkpoint inhibitors like ipilimumab represents one of the most significant advancements in oncology, offering hope for patients with previously untreatable malignancies.
Related: HTP Recombinant Antibody Production
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including HTP Recombinant Antibody Production, Bispecific Antibody Production, Large Scale Antibody Production, and Afucosylated Antibody Expression. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Saad, P., & Kasi, A. (2023, April 10). Ipilimumab. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557795/
UC Berkeley Cancer Research Lab» The Story of Yervoy (Ipilimumab). (2025). Berkeley.edu. https://live-cancer-research-lab.pantheon.berkeley.edu/discoveries/the-story-of-yervoy-ipilimumab/
Rowshanravan, B., Halliday, N., & Sansom, D. M. (2017). CTLA-4: A moving target in immunotherapy. Blood, 131(1), 58. https://doi.org/10.1182/blood-2017-06-741033
Two popular topics discussed at the 2026 BIO International Convention were devel……
AI is changing antibody discovery, but model performance depends on the quality ……
Antibody discovery has become increasingly sequence-rich. Display technologies, ……
Biointron, a leading contract research organization specializing in antibody dis……